

Abstract
Since 2001, a synthesizing element in Intergovernmental Panel on Climate Change assessment reports has been a summary of how risks in a particular system could change with additional warming above pre-industrial levels, generally accompanied by a figure called the burning embers. We present a first effort to develop burning embers for climate change risks for heat-related morbidity and mortality, ozone-related mortality, malaria, diseases carried by Aedes sp., Lyme disease, and West Nile fever. We used an evidence-based approach to construct the embers based on a comprehensive global literature review. Projected risks for these health outcomes under 1.5 °C, 2 °C, and >2 °C of warming were used to estimate at what temperatures risk levels increased from undetectable to medium, high, and very high, from the pre-industrial baseline, under three adaptation scenarios. Recent climate change has likely increased risks from undetectable to moderate for heat-related morbidity and mortality, ozone-related mortality, dengue, and Lyme disease. Recent climate change also was assessed as likely beginning to affect the burden of West Nile fever. A detectable impact of climate change on malaria is not yet apparent but is expected to occur with additional warming. The risk for each climate-sensitive health outcome is projected to increase as global mean surface temperature increases above pre-industrial levels, with the extent and pace of adaptation expected to affect the timing and magnitude of risks. The embers may be an effective tool for informing efforts to build climate-resilient health systems including through vulnerability, capacity, and adaptation assessments and the development of national adaptation plans. The embers also can be used to raise awareness of future threats from climate change and advocate for mitigation actions to reduce the overall magnitude of health risks later this century and to expand current adaptation efforts to protect populations now.
Export citation and abstract BibTeX RIS

Original content from this work may be used under the terms of the Creative Commons Attribution 4.0 license. Any further distribution of this work must maintain attribution to the author(s) and the title of the work, journal citation and DOI.
Abbreviations
| IPCC | Intergovernmental Panel on Climate Change |
| RFC | Reasons For Concern |
| SSPs | Shared Socioeconomic Pathways |
| UNFCCC | United Nations Framework Convention on Climate Change |
1. Introduction
The long-term objective of the UNFCCC is to prevent dangerous anthropogenic interference with the climate system (UNFCCC 1992). Article 2 of the Convention states that interference would not be dangerous if greenhouse gas emissions were stabilized at levels that will ensure that ecosystems have time to adapt naturally; that food production is not threatened; and that economic development can proceed in a sustainable manner (UNFCCC 1992). The question to the scientific community was how to quantify dangerous interference in ways that would be consistent, repeatable, and comparable over time, understanding that what is considered dangerous is a socially held value.
To inform negotiations on the level of ambition of greenhouse gas emission reductions consistent with this purpose, Smith et al (2001) synthesized climate change risks to enable readers to 'evaluate the relationship between increases in global mean temperature and impacts.' The authors identified five aggregate RFC to facilitate public discussions and policy decisions pertaining to what is dangerous climate change. The assessment determined what temperature above pre-industrial temperatures increased the risk level, in steps from undetectable to very high. RFCs can be used individually or in combination to understand the relationship between global mean temperature increase and:
- (a)damage to or irreparable loss of unique and threatened systems (e.g. tropical glaciers, coral reefs, mangroves, and biodiversity hot spots);
- (b)distribution of impacts (e.g. income inequality);
- (c)global aggregate market and non-market damages;
- (d)probability of extreme climate effects (e.g. extreme weather and climate events); and
- (e)probability of large-scale singular events such as the breakup of the West Antarctic Ice Sheet or the collapse of the North Atlantic thermohaline circulation.
For each RFC, a companion figure (burning ember) showed the temperature range at which risk levels change; the transitions were determined by a combination of assessment of the scientific literature and expert judgment of the author team and reviewers. The baseline was pre-industrial temperatures.
Subsequent IPCC assessment reports updated the diagram to reflect new scientific evidence and insights, showing that risks were projected to be greater and to occur sooner than described in the previous assessment cycles (Schneider et al 2007, Oppenheimer et al 2014, Smith et al 2009, Hoegh-Guldberg et al 2018, IPCC 2019a, IPCC 2019b). The IPCC Special Report on Climate Change and Land developed the method further by conducting expert elicitations to determine the temperature transitions where risk increased from undetectable through to very high (Zommers et al 2020).
This framework and diagram are iconic elements of IPCC assessment reports, used to inform policy by communicating climate change-related risks in an easily understandable and accessible manner. There is growing interest in incorporating considerations of vulnerability and adaptation into the embers, and the concept has been extended to apply to several specific systems. In 2015, Gattuso et al applied the framework to summarize the risks of elevated concentrations of carbon dioxide and climate change on coastal and marine organisms and ecosystem services, summarizing how risks to, for example, warm water corals and fin fish, are projected to increase with climate change. Hoegh-Guldberg et al (2018) in the IPCC Special Report on Global Warming of 1.5 °C included the first ember for a climate-sensitive health outcome: heat-related morbidity and mortality. We update the comprehensive literature review in Ebi et al (2018) on the projected health risks of warming of 1.5 °C and higher to construct health embers for six health outcomes. We complement the evidence-based assessment with expert judgment to assess the likely future risks under different assumptions of socioeconomic development.
2. Methods
We used an evidence-based approach to construct the embers, based on projections of health risks under 1.5 °C, 2 °C, and >2 °C of warming, for heat-related morbidity and mortality; mortality related to exposure to ozone; and the geographic distribution, vectorial capacity, or mortality associated with dengue; Lyme disease; malaria; and West Nile virus. We first updated the Ebi et al (2018) comprehensive review of the projected health risks of climate change, particularly the table documenting the projected changes in risk at 1.5 °C and 2 °C to include projections of risks at >2 °C of warming, and to add literature published through June 2020. The same search terms and databases were used for the update; see annex 1 in supplementary material (available online at stacks.iop.org/ERL/16/044042/mmedia) for the search terms and tables summarizing projections for each health outcome included.
The assessment was global, drawing on worldwide literature. We did not attempt to construct burning embers for geographic regions because there were insufficient projections at finer scales to support robust evidence-based assessments. We note that levels of risk of different health threats can be very different in different regions and can respond very differently to efforts to build health system resiliency, including levels of adaptive capacity.
Because most health projections were for time periods (e.g. 2050s, 2080s), not temperatures, time periods were converted to expected warming as in Ebi et al (2018) (see tables in supplementary materials). The diversity in study approaches and methods meant it was not possible to combine the projections into a meta-analysis, and few projections considered possible future adaptation.
The projections of health risks by temperature were used by the authors to judge when the level of risk of specific outcomes could change substantially, drawing on present understanding of the role of temperature in the exposure pathway. As detailed in the supplementary tables, temperature is directly associated with heat-related morbidity and mortality. Temperature alters exposure pathways in more complex ways for ozone and the four vector-borne diseases assessed. We used the risk transitions defined for other burning ember diagrams (see table 1 for definitions). Because of the limited number of detection and attribution studies (e.g. Mitchell et al 2016, Ebi et al 2017), the author team agreed on the temperature at which there was or likely would be a transition from undetectable to moderate risk (e.g. white to yellow). If a risk was judged to have changed from moderate (yellow) to substantial (red), then the transition was assumed to occur approximately halfway between the starting (e.g. 1.5 °C) and ending temperature (e.g. 2 °C). Because of the limited projections for global mean temperature increases above 2 °C, the author team discussed and agreed on transitions at higher degrees of warming. There are differences in risk among the health outcomes, as would be expected, because of different thresholds and non-linearities in relation to temperature increase and levels of adaptation.
Table 1. Risk transitions and associated colors used in the embers diagram.
| Color | Risk | Definition |
|---|---|---|
| White | Undetectable | No impacts/risks detectable and attributable to climate change |
| Transition to yellow | Low | Impacts/risks detectable and attributable to climate change |
| Yellow | Moderate | Impacts/risks detectable and attributable to climate change with at least medium confidence |
| Transition to red | Substantial | Substantial impacts/risks attributable to climate change |
| Red | High | Severe and widespread impacts/risks attributable to climate change |
| Purple | Very high | Even more severe and widespread, irreversible, or persistent impacts/risks attributable to climate change with the presence of significant irreversibility, combined with limited ability to adapt |
Source: Hoegh-Guldberg et al (2018).
Once the transitions between risk categories were determined, the authors then agreed on the level of confidence in each transition. The IPCC approach to determining the confidence in key findings in the 5th Assessment Report was used (IPCC 2010). Confidence was based on an evaluation of the extent of evidence (amount, quality, and consistency, ranked as limited, medium, or robust) and the level of agreement across the projections (low, medium, and high). The level of confidence was expressed using five qualifiers: very low, low, medium, high and very high. The embers are based on global averages unless otherwise noted, assuming average susceptibility within each adaptation level.
The embers were drawn using the 'Embers Factory' ≪https://climrisk.org/emberfactory≫.
2.1. Adaptation scenarios
We consider three levels of adaptation based on the SSPs (O'Neill et al 2017, Sellers and Ebi 2018): worlds in which adaptation would: fall behind in preventing avoidable climate-sensitive morbidity and mortality (SSP3); continue the current development trend with slowly improving adaptation (SSP2); and aim for sustainable development where adaptation is more effective than today in preventing adverse climate-sensitive health outcomes (SSP1). Table 2 lists some of the characteristics of health systems under the three SSPs. We assumed that projections that did not explicitly consider adaptation followed a SSP2 pathway.
Table 2. Selected characteristics of health systems under the shared socioeconomic pathways.
| SSP3 | SSP2 | SSP1 | |
|---|---|---|---|
| Basic characteristics | Reactive; failure to adapt; siloed information channels and national governance; limited partnerships | Incomplete planning; new information incorporated as convenient; occasional partnerships | Proactive; adaptively managed; frequent partnerships; interdisciplinary |
| Building blocks of health systems | |||
| Leadership and governance | Little focus at national and international levels on climate change and health; minimal planning conducted | Planning on climate change and health, but not comprehensive and often sidetracked by other issues | Strong climate change and health planning apparatus, including health components of national adaptation plans; regional/international partnerships |
| Health information systems | Vulnerability and adaptation assesssments rarely, if ever conducted; information not useful for planning; minimal risk monitoring or climate change and health research | Vulnerability and adaptation assessments occasionally conducted, but generally of poor quality; early warnings incomplete; fiscal and political constraints on climate change and health research | Vulnerability and adaptation assessments regularly conducted and used in planning; robust early warning networks; research agenda focused on vulnerable communities |
| Climate resilient and sustainable technologies and infrastructure | Facilities sited and constructed without climate consideration incorporated; medical supply chains not modified | Capital cost serves as key factor in siting and construction; increasing vulnerability of facilities to shocks | Health infrastructure designed to be robust to storms/floods, with redundant systems added to ensure continuity of care |
| Service delivery | Policies to manage environmental health hazards generally not followed; care practices not modified to accommodate climate information; few changes to emergency management procedures; health inequities worsen | Environmental health policies are not robust; marginal improvements in care practices; risk assessments and communication inadequate; no shift in health inequities | Policies to manage environmental health hazards regularly reviewed; practitioners review care practices and adjust as appropriate based on local climate and health conditions; robust communication tools developed; health service improvements reduce health inequities |
| Health system objectives | Unaccountable, inefficient, inequitable, low-quality, vulnerable, unsustainable | Intermittent accountability, moderate efficiency, fair quality, variable resilience, moderately sustainable | Accountable, efficient, equitable, high-quality, resilient, sustainable |
Source: modified from Sellers and Ebi (2018).
We expect health systems would continue to take action to prepare for and manage the risks of climate change. But the speed at which challenges were recognized and addressed would follow the pathways described in table 2. For example, under SSP3, policies proven effective in other jurisdictions could be implemented too late to achieve their objectives, thus exposing populations to greater hazards with insufficient programs and technologies to prevent avoidable morbidity and mortality.
The transition points for each health outcome for low (SSP3) and high adaptation (SSP1) were judged by the author team on the basis of their collective expertise, taking into account each of the development pathways. Some health authorities have begun taking measures to prepare for climate change but, in many respects, most health systems worldwide presently have low adaptation, with localized, incremental, and generally disjointed activities (Smith et al 2014, Hess and Ebi 2016, UNEP 2018), aligned generally with characteristics of SSP3. In theory, this provides a reference point or counterfactual for the future levels of adaptation of health systems. However, because health systems are constantly evolving, generally but not always improving, it would be inappropriate to assume that health systems would make no additional efforts to manage climate-related health risks as the climate continues to change.
Looking ahead, health models could be improved by incorporating a range of possible adaptation pathways, based upon studies of observed adaptation, to provide greater insights into the extent to which these pathways could reduce future risks.
3. Results
The tables in supplementary materials provide a basic description for each study included in the assessment, including the health outcome metric used, the study baseline, climate model(s), scenario, time periods of interest, projected impacts at 1.5 °C, 2 °C, and >2 °C, and other factors considered. There were 40 studies published since Ebi et al (2018). There were three new studies in addition to the thirty-four studies included in Ebi et al (2018) projecting heat-related mortality (Lee et al 2019, Varquez et al 2020, Zhang et al 2020); four new studies projecting ozone-related mortality (Heal et al 2013, Stowell et al 2017, Chen et al 2018, Chowdury et al 2018). There were five new studies in addition to the ten in Ebi et al (2018) projecting changes in the geographic range of the malaria vector or numbers of people at risk of malaria (Laporta et al 2015, Kibret et al 2016, Ren et al 2016, Akpan et al 2019, Ryan et al 2020). There were 19 new studies projecting changes in the geographic range of the mosquito vector or intensity of transmission of dengue fever, Zika virus, chikungunya, and yellow fever (Colon-Gonzalez et al 2013, Henry and Mendonca 2020, Liu et al 2019a, Liu et al 2019b, Proestos et al 2015, Butterworth et al 2017, Monaghan et al 2018, Carbajo et al 2019, Jing-Chun et al 2019, Kramer et al 2019, Messina et al 2019, Ryan et al 2019, Cabrera et al 2020, Iwamura et al 2020, Kakala et al 2020, Khan et al 2020, Rohat et al 2020, Sintayehu et al 2020, Tran et al 2020). These are in addition to the 19 studies in Ebi et al (2018). There were four new studies in addition to the eight in Ebi et al (2018) projecting the geographic distribution and onset of Lyme disease (Monaghan et al 2015, Alkishe et al 2017, Li et al 2019, MacDonald et al 2020). And finally, there were five new studies in addition to the six in Ebi et al (2018) projecting changes in West Nile fever or its vector (Morin and Comrie 2013, Harrigan et al 2014, Paull et al 2017, Bhowmick et al 2020, Gangoso et al 2020). There were fewer projections for other health risks, such as undernutrition and impacts of heat stress on occupational health, and so are not included.
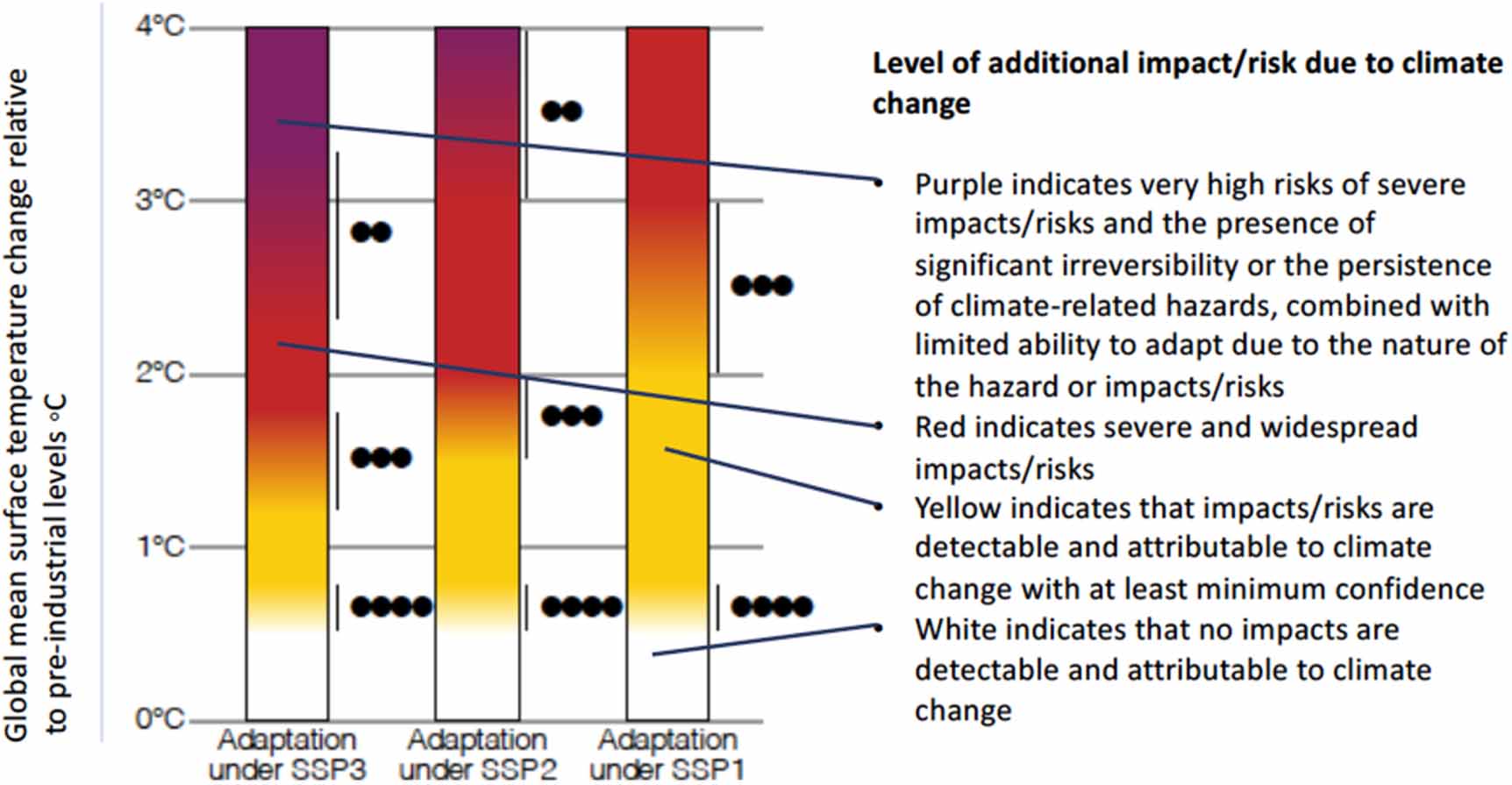
To illustrate how the levels of additional impact/risk due to climate change are graphically represented in the ember diagrams, figure 1 shows the details for heat-related morbidity and mortality. Figure 2 shows the burning embers under three adaptation scenarios for heat-related morbidity and mortality, ozone-related mortality, malaria, dengue and other diseases carried by Aedes mosquitoes, Lyme disease, and West Nile fever.

Figure 1. Details of burning embers for heat-related morbidity and mortality. The dots show the confidence in the transitions, with four dots very high confidence, three dots high confidence, two dots medium confidence, and one dot low confidence.
Download figure:
Standard image High-resolution image
{kind=link}
Figure 2. Burning embers for health under three adaptation scenarios. The dots show the confidence in the transitions, withfour dots very high confidence, three dots high confidence, two dots medium confidence, and one dot low confidence.
Download figure:
Standard image High-resolution image{kind=link}
As expected from Hoegh-Guldberg et al (2018), heat-related morbidity and mortality increased with projected temperature increase, with risks higher under SSP3 than SSP1. Detection and attribution studies (Mitchell et al 2016, Ebi et al 2017, 2020) show that climate change is already causing additional deaths during heatwaves; therefore, the risk transition shifted from undetectable (white) to moderate (yellow) before 1 °C of warming. Because most heat-related deaths are preventable (Hajat and Kosatsky 2010) and because heatwave early warning systems, based on heatwave action plans, have been demonstrated to reduce mortality (Fouillet et al 2008), we assumed that adaptation under SSP2 would delay the risk transition from moderate to high (red) until global temperatures increased to 2 °C. The transition time to higher risk was longer under SSP1 and shortened under SSP3. Risk is expected to transition to very high (purple) as temperatures rise to 3.5 °C under SSP2 and 3 °C under SSP3, based on the range of temperatures within which human physiological responses are effective in maintaining core body temperature (Vanos et al 2020). The ability to successfully manage heat-related morbidity and mortality will be increasingly challenged with higher degrees of warming, particularly in circumstances that amplify heat risks, including where high temperatures are accompanied by high humidity and increased exposures render public health interventions less effective (Woodward et al 2020).
The embers for ozone-related mortality show a similar pattern to those for heat-related morbidity and mortality because ozone formation is temperature-sensitive, although the risk transitions are at lower temperatures because there are far fewer adaptation options with increasing challenges to adaptation in SSP3. The underlying projections assumed that precursor emissions will remain constant; if regulations reduce precursor emissions, then the embers would likely overestimate the levels of risk. Embers were not created for mortality related to particulate matter because of the uncertainty of how climate change could affect atmospheric concentrations (Ebi and McGregor 2008).
Embers were created for four vectorborne diseases: malaria, dengue and other diseases carried by Aedes sp., Lyme disease, and West Nile fever. Weather, particularly temperature, and other environmental variables are key factors determining the distribution of their vectors and the months over which they are active (Brugueras et al 2020).
Creating embers for malaria took into account that some regions may become too hot and/or dry for the Anopheles mosquito with additional warming. Therefore, even though risks are projected to increase overall at higher levels of warming, they may not increase everywhere and may even be reduced in some regions. The complexity of the malaria transmission cycle and the presence of multiple drivers of malaria incidence mean that it has not yet been possible to detect a change in malaria that can be attributed to climate change. The assessed projections indicate the impact of climate change could be evident within another half degree of warming and rise steadily with higher temperatures because of further shifts in the geographic distribution, seasonality, and intensity of transmission. This is consistent with malaria increasing in many African countries (WHO 2020). It is too early to determine whether climate change is affecting increases in the geographic range of an Asia Anopheles mosquito involved in a recent outbreak of malaria in Djibouti City (Sinka et al 2020); if this is the case, then temperature transitions may be underestimated. The challenges associated with developing and delivering an effective vaccine for malaria mean that risk is expected to increase even under SSP1.
Large outbreaks of dengue fever occurred worldwide in 2019–2020. Three million cases occurred in the Americas alone in 2019, over double the number of cases that occurred annually over previous years (PAHO 2020). Over 2 million cases occurred through September 2020. Outbreaks also were recorded in multiple countries in the Western Pacific Region of WHO (WPRO 2020), raising concerns that climate change was contributing to the increase in the geographic range and number of months that the mosquito species that carries dengue, Aedes sp., is active (Ryan et al 2019).
These mosquitoes also can carry yellow fever, Chikungunya, and Zika viruses. As with malaria, the risk transitions took into account that some regions may become too hot and/or dry for the mosquito in some regions with additional warming. Climate change may be one reason for recent changes in the geographic range of Aedes sp. (Sukhralia et al 2019), supporting the risk transition from undetectable to moderate before 1 °C of warming. Indeed, local transmissions of Chikungunya and Zika have been confirmed during the last years in Euro-Mediterranean countries (World Health Organization 2017). The responsiveness of the vector to additional warming and the potential for vector control programs to address changes in risk suggests that under SSP2, risk could transition from moderate to high with another degree of warming, with the risk continuing to climb with additional warming. Greater (SSP3) or fewer (SSP1) challenges to adaptation would shift the temperature at which risk transitions occurred (down and up, respectively).
A detection and attribution study suggested that climate change has already affected the geographic distribution and numbers of cases of Lyme disease in Canada (Ebi et al 2017); therefore, the risk transition from undetectable to moderate was before 1 °C of warming. The responsiveness of the vector to additional warming suggests that under SSP2, risk could transition from moderate to high with another half degree of warming, with the risk continuing to climb with additional warming. Additional investments in adaptation, such as enhancing surveillance and monitoring systems, could delay the increase in risk under SSP1; the lack of such measures would fail to reduce risks to health under SSP3.
Climate change has apparently already affected the geographic range of West Nile fever. Since emerging in southern and eastern Europe during the summer of 2010 following a severe heatwave, there have been annual outbreaks, suggesting an endemic transmission cycle and thus a resurgent public health problem (Paz 2015). In 2018, the virus was detected for the first time in Germany (Kampen et al 2020). Under SSP2, risk was assessed to increase to moderate starting at 1.5 °C of warming and to further increase with additional warming. As with the other vectorborne diseases, risk transitions were assessed to occur sooner under SSP3 and take longer under SSP1 due to more aggressive adaptation measures and greater resiliency of health systems.
4. Discussion
This first effort to develop burning embers for multiple health risks of climate change shows both the extent to which risks could increase with higher ambient temperatures and the opportunities for proactive adaptation under SSP1 to reduce those risks. As expected, global risks are projected to increase as temperatures increase above pre-industrial levels. Climate change likely has already increased risks from undetectable to moderate for heat-related morbidity and mortality, ozone-related mortality, dengue, and Lyme disease. Recent climate change was assessed as possibly beginning to affect the burden of West Nile fever.
The available literature is more focused on projecting risk than quantifying the numbers of cases, although the Y axis of the embers diagrams suggests interchangeability. Risks and impacts are correlated but the relationship is variable across the health outcomes assessed. For instance, risks related to heat-related morbidity and mortality are highly correlated with impacts. For mosquito-borne disease, the literature is more focused on populations at risk or the geographic range of the vector than on projecting numbers of additional cases of disease. At lower levels of risk, transitions from undetectable to detectable and attributable can occur without widespread impacts. Risks can increase due to the presence of a hazard and some degree of population exposure and susceptibility. As risks increase, so could impacts, particularly when large populations are susceptible and exposed. This is particularly likely with novel hazards for which current adaptation is minimal and opportunities to expand such efforts are limited or face barriers, for example, due to limited resources or technologies.
Risk transitions differ across the SSPs, with the transitions occurring at lower temperatures under SSP3 and at higher temperatures under SSP1, illustrating the extent to which the strength of health systems is likely a critical determinant of the magnitude of future health risks. However, these descriptions of adaptive capacity are qualitative and have not been quantified as input into model projections. Projections based on these quantifications are needed to verify the accuracy and usefulness of the proposed scenarios. If accurate, they illustrate the imperative for strengthening health systems, with sufficient adaptive capacity to prepare for and manage health risks as the climate continues to change.
The effectiveness of adaptation may not be symmetric with increasing temperatures. The difference between a well-adapted world and a poorly adapted world for the health of individuals and communities may be most marked with moderate warming (around the yellow to red zone). Adaptation matters less (in relative terms) when the threat of impacts is slight and becomes more important as the threat increases. At higher levels of warming, adaptation becomes increasingly marginal as risks increase further and limits to adaptation are approached. This can be illustrated by the impact of air conditioning; access does not matter much when it is not so hot but becomes more significant as temperatures rise along with health risks. Eventually at very high temperatures, air conditioning can become unreliable if power grids buckle under increased demand. Air conditioning may not be fit for purpose as a primary form of adaptation at very high temperatures.
The complexity and diversity of possible challenges in adapting, as highlighted in the SSPs, mean that progress in protecting health is unlikely to be smooth, even for jurisdictions that begin early and aggressively. Health authorities that lack the capacity to build climate resilient health systems, or are delayed in implementing needed measures, will have to address significantly higher risk levels as the climate continues to warm. The starting point makes a difference—one might expect the level of adaptation would make more of a difference in protecting health in the short term, particularly if the health system and population are unprepared and are more vulnerable to impacts. Awareness, a sense of urgency, and opportunities to act will not be evenly distributed across the full range of warming. At lower temperature changes, there may not be sufficient incentive to make significant change; higher temperatures will demonstrate the necessity, but adaptation may be too constrained or too late. In addition, the requirements and resources for well-planned and proactive adaptation to protect health may become increasingly constrained as individuals and health systems must cope with greater impacts at higher levels of warming.
On the other hand, a progression from medium to high adaptation might amplify benefits and protection through the creation of synergies and co-benefits of actions. For example, regular assessments that inform the siting of climate resilient infrastructure with redundancy in the case of disasters and support by adequate levels of funding would heighten preparedness of the health sector for a range of climate and non-climate related hazards. In this case, risks might not move from yellow to red until higher temperatures in the high adaptation scenario.
A strength of the study is that the embers are based on published projections, at least under SSP2. Study limitations include the use of expert judgment to estimate the risk transitions under SSPs 1 and 3 and the limited numbers of projections at higher degrees of warming. It would be helpful to compare the results of this assessment with a formal expert elicitation process similar to that used by Zommers et al (2020).
We suggest the embers may be an effective communication tool that can be used by health organizations and institutions, such as the World Health Organization and its regional offices, other UN organizations, ministries and departments of health, and other health decision-makers, to inform vulnerability, capacity, and adaptation assessments, the development of plans to build climate-resilient health systems, and national adaptation priorities. The embers also can be used to advocate for mitigation to reduce the overall magnitude of risks later this century and for accelerated adaptation actions to delay risk transitions for as long as possible. Most embers are global averages, and these could, with due caution, be downscaled to regional or national levels using expert judgment until more projections are available. Doing so would provide national and local decision-makers greater insights into challenges the populations they serve, and their healthcare systems, could be expected to face.
Acknowledgments
Ms Marci Burden, MA.
Data availability statement
All data that support the findings of this study are included within the article (and any supplementary files).