
Abstract
As a vibrator needs to be pressed onto the osseous parts of the head, bone conduction is often accompanied by pain and esthetic problems. To solve these problems, a "distant presentation" that involves presenting vibrators to the neck, trunk, or upper limb was proposed. Our previous studies focused on the perceptual and propagation characteristics of distantly presented bone-conducted sounds in the ultrasonic range. However, only a few studies have been conducted in the audible-frequency range. In this study, to examine the basic properties of distantly presented bone-conduction perception in the audible-frequency range, hearing thresholds, difference limens for frequency, and temporal modulation transfer functions were measured with insulated air-conducted sounds. The results indicate that the distance attenuation is much larger than that in the ultrasonic range, and the degradation of frequency and temporal information occurring in the propagation process of bone-conducted sounds is sufficiently small for the transmission of sound information.
Export citation and abstract BibTeX RIS
1. Introduction
Sounds are usually perceived as vibrations of air. This is referred to as air conduction. However, we can perceive sound even as a vibration of biological tissues (bone, skin, muscle, etc.), which is called bone conduction. Bone conduction is an effective way to restore hearing acuity in patients with conductive hearing impairment. Furthermore, bone conduction has recently been applied to more general audio interfaces, such as earphones, taking advantage of the fact that the external auditory canal does not need to be obstructed.
Although the upper-frequency limit of human hearing is believed to be approximately 20 000 Hz, several studies have reported that high-frequency sound up to at least 100 000 Hz can be perceived clearly via bone conduction. 1–3) This "audible" ultrasound through bone conduction is referred to as bone-conducted ultrasound (BCU). BCU hearing in humans has been demonstrated under various auditory pathological conditions, such as middle ear disorders and sensorineural hearing impairment. 3) This is true even for the profoundly sensorineural-hearing-impaired, who can hardly sense sounds even with conventional hearing aids. 4,5) Furthermore, BCU amplitude-modulated by speech sounds is intelligible to some extent; thus, BCU has been applied as a novel hearing aid for the profoundly sensorineural-hearing-impaired (BCU hearing aid: BCUHA). 6–8)
The perceptual mechanisms of BCU have been investigated in various studies. Previous electrophysiological measurements indicated that the ordinary auditory pathway, from the brainstem to the auditory cortex, is activated by BCU, and there is no special organ that receives ultrasound. 9–11) Moreover, previous psychophysical measurements of the pitch, 2,12–14) the masking effect, 15) and the dynamic range of loudness of BCU perception 15) have shown that some differences exist between the perception of sounds in the audible-frequency range and that of BCU in the inner ear, although the cochlea contributes to BCU perception. On the other hand, several reports have indicated that the BCU presented could be converted into an audible sound in the head. 16,17) However, evidence for the generation of audible-frequency components associated with the presentation of BCU has not been obtained from physioacoustical and optical measurements. 18,19)
Generally, in bone-conduction devices, including BCUHA, the vibrator needs to be pressed onto the osseous parts of the temporal bone behind the ear, such as the mastoid process. Therefore, bone conduction is often accompanied by pain and esthetic problems. Additionally, holding the vibrator steadily on the round surface of the mastoid process is difficult. Thus, "distant presentation" has been proposed to solve these problems. 20) The distant presentation involves presenting vibrators to the muscles of the neck, trunk, or upper limb, and is believed to rectify the disadvantage of conventional bone-conduction devices.
We have studied the perceptual and propagation characteristics of distantly presented BCU and its application to a novel audio interface. 20–23) Nakagawa et al. measured hearing thresholds when 30 000 Hz tone bursts were presented to the neck, and upper and lower arms and estimated temporal modulation transfer functions (TMTFs), which reflect the temporal resolution of human hearing, for a distantly presented 30 000 Hz carrier to assess the basic properties of distantly presented BCU hearing. The results showed that the thresholds increased depending on the propagation distance and that the temporal resolution of BCU hearing presented to the distal parts of the body was comparable to that presented to the mastoid process. 20) Ogino et al. measured the vibrations on the body surface and in the external auditory canal when 30 000 Hz tone bursts were presented to the distal parts. They showed that the vibration decreased depending on the distance between the stimulus placement and the measurement point and that the efficiency of the BCU transmission appears to vary depending on factors, such as the shape and acoustical properties of the tissue, and coupling between the vibrator and skin. 21) In addition, our previous studies on the perceptual and propagation characteristics of amplitude-modulated BCU presented to the distal parts indicated that the demodulation components, which were generated due to the biological tissues with nonlinearity present in the propagation process of amplitude-modulated BCU, can be used to improve the hearing of the distantly presented BCU. 22,23)
However, only a few studies have been conducted on distantly presented bone conduction in the audible-frequency range. 24,25) Analysis in the audible-frequency range to elucidate the essential mechanisms of the perception and propagation of bone-conducted sounds presented to the distal parts is indispensable.
In the ultrasonic range, only the perception of bone-conducted sound components can be evaluated because air-conducted sound components radiated from the vibrator are never perceived. In contrast, in the audible-frequency range, not only bone-conducted sounds but also air-conducted sounds radiated from the vibrator are perceived. Therefore, air-conducted sounds need to be sufficiently insulated to evaluate only the perception of bone conduction.
In this study, hearing thresholds were measured, as a first step to verify the basic perceptual characteristics of distantly presented bone-conducted sound in the audible-frequency range. Furthermore, to assess the characteristics of transferring frequency and temporal information, difference limens for frequency (DLFs), which reflect the frequency resolution of human hearing, and TMTFs were measured. In all the measurements, the air-conducted sounds radiated from the vibrator were sufficiently insulated.
All the experiments conducted in this study were approved by the Institutional Review Board of Life Science Research of Chiba University. Necessary information about the experiments was provided to the participants, and informed consent was obtained from each participant before the experiments.
2. Experimental methods
2.1. Insulation of air-conducted sounds with earplug and earmuff
In this study, air-conducted sounds were insulated strongly by two types of earplugs and an earmuff to evaluate only the bone-conduction components. First, urethane earplugs (DKSH Japan Silencia) were inserted into the external auditory canals of the subjects. Subsequently, ear conchae were covered with silicone earplugs (Insta-Mold Products Insta-Putty). Finally, except when the stimulus was presented to the mastoid process, the participants wore an ear-muff (3 M PELTOR X5A) over the earplugs (Fig. 1). To examine the insulating effect, we measured the sound pressure level of the air-conducted sounds radiated from the vibrator at the opening of the external auditory canal and the sound attenuation value of the insulating method used in this study based on ISO 4869. 26)
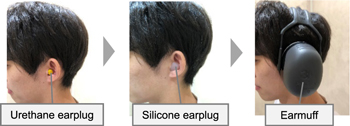
Fig. 1. (Color online) Method of insulation of the air-conducted sounds used in the experiments.
Download figure:
Standard image High-resolution image2.1.1. Measurement of the sound pressure level of air-conducted sounds at the opening of the external auditory canal
The sound pressure level was measured at the opening of the external auditory canal when the bone-conduction stimulus was presented under the same conditions as the DLF and TMTF measurements to evaluate the amount of air-conduction component radiated from the vibrator reaching the ear in the DLF and TMTF measurements. One male (23 years old) with no history of deficits in his hearing functions participated.
As stimuli, 1000, 2000, 3000, and 4000 Hz tone bursts presented at 15 dB SL, and 1000 Hz and 4000 Hz tone bursts presented at 25 dB SL were used. The sound pressure level was measured using a binaural microphone (Bruel and Kjaer 4101) on the left side of the opening of the external auditory canal when these stimuli were presented to the left side of the following body parts: (a) the mastoid process of the temporal bone, (b) sternocleidomastoid muscle (muscle of the neck; middle point between the mastoid process and the sternoclavicular joint), and (c) the sternal end of the clavicle (except when the 4000 Hz tone burst was presented at 25 dB SL).
2.1.2. Estimation of the sound attenuation value based on ISO 4869
The sound attenuation value was estimated based on ISO 4869 to evaluate the insulation performance of the insulating method used in this study. 26)
Ten adults (9 males and 1 female, 21–26 years) who had no history of deficits in their hearing functions participated. The stimuli consisted of pink noise filtered through one-third octave bands with the center frequencies (CFs) of 1000, 2000, 3000, and 4000 Hz (duration: 800 ms). These stimuli were presented using a loudspeaker (Genelec 8010 A) installed in front of the participant at a distance of 1 m.
The hearing thresholds were measured with and without the insulation to estimate the sound attenuation value. The difference between the hearing thresholds at each CF was defined as the sound attenuation value. The hearing thresholds were measured using a two-up one-down three-alternative forced-choice (3AFC) adaptive procedure (details will be provided in Sect. 2.2.1).
2.2. Setup for the experiments examining the basic properties of distantly presented bone conduction
Seven males (21–26 years) with no history of deficits in their hearing functions participated. Bone-conduction stimuli were presented to the left side of the following body parts (Fig. 2): (a) the mastoid process of the temporal bone, (b) sternocleidomastoid muscle, (c) the sternal end of the clavicle, and (d) acromion (only for the hearing threshold measurement). Bone-conduction stimuli in the audible-frequency range (audible stimuli) were presented using a bone-conduction vibrator [RadioEar B-81, Fig. 3(a)], and bone-conduction stimuli in the ultrasonic range (ultrasonic stimulus) were presented using a piezoelectric ceramic vibrator [Murata Manufacturing MA40E7S, Fig. 3(b)]. Figure 4 shows the frequency response for B-81 used in this study between 100 and 10 000 Hz at a constant input voltage of 1 VRMS.

Fig. 2. Stimulus placements used in the experiments: (a) mastoid process of the temporal bone, (b) sternocleidomastoid muscle (muscle of the neck; middle point between the mastoid process and the sternoclavicular joint), (c) sternal end of the clavicle and (d) acromion.
Download figure:
Standard image High-resolution image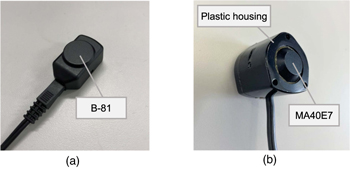
Fig. 3 Bone-conduction vibrators used in the experiments. (a) Bone-conduction vibrator (RadioEar B-81) used in all the experiments to present bone-conducted sounds in the audible-frequency range. (b) Bone-conducted ultrasound (BCU) vibrator used in the measurement of hearing thresholds. A piezoelectric ceramic vibrator (Murata Manufacturing MA40E7S) was covered by a plastic housing.
Download figure:
Standard image High-resolution image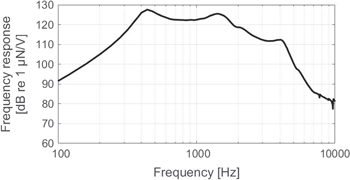
Fig. 4. Frequency response for the B-81 used in the experiments measured at an input voltage of 1 VRMS from 100 to 10 000 Hz. The magnitude is given in decibels relative to 1 μN V−1.
Download figure:
Standard image High-resolution imageThe audible stimuli were generated with a personal computer using MATLAB (MathWorks) at a sampling frequency of 48 000 Hz and fed to the vibrator via a 24 bit D/A converter (Echo Digital Audio Audiofire 12). On the other hand, the ultrasonic stimuli were generated with a personal computer using MATLAB at a sampling frequency of 192 000 Hz and fed to the vibrator via a 24 bit D/A converter and amplifier (Mess-Tek M-2629B). The bone-conduction vibrators were pressed onto the mastoid process and sternocleidomastoid muscle using an elastic band with foam [Figs. 5(a) and 5(b)]. An icing supporter was used to fix the vibrator to the clavicle and acromion [Figs. 5(c) and 5(d)].
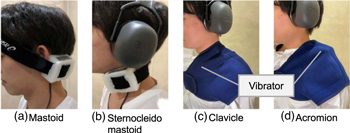
Fig. 5. (Color online) Fixed locations of the vibrator in the experiments. An elastic band with foam was used to fix the vibrator to the (a) mastoid process and (b) sternocleidomastoid muscle, and an icing supporter was using to fix the vibrator to the (c) clavicle and (d) acromion. 25)
Download figure:
Standard image High-resolution imageJust prior to the experimental sessions in each measurement, the stimulus was presented at the stimulus intensity of the measurement (described later) with the vibrator slightly away from each stimulus location. Then it was confirmed that the air-conducted sounds radiated from the vibrator were not perceived by participants subjectively at any frequency. All the measurements were conducted in an anechoic room.
2.2.1. Measurement of hearing thresholds
The hearing thresholds were measured when the bone-conduction stimuli were presented to the head (mastoid process), neck (sternocleidomastoid), trunk (clavicle), and shoulder (acromion).
As the audible stimuli, 250, 500, 750, 1000, 2000, 3000, and 4000 Hz tone bursts with a duration of 800 ms, including 75 ms rising/falling ramps, were used. In addition, a 30 000 Hz tone burst with a duration of 800 ms, including a 75 ms rising/falling ramp, was used as the ultrasonic stimulus to compare the hearing threshold of bone-conducted sound in the audible-frequency range with that in the ultrasonic range.
The hearing thresholds were measured using a two-up one-down 3AFC adaptive procedure with a decision rule that estimated the 70.7% correct point on the psychometric function. 27) In this procedure, three intervals were presented sequentially, and the stimulus was presented only in one of the three intervals. The participants were requested to respond to a section in which the sound was perceived. The hearing threshold measurements were started from the stimulus intensity at which the sound could be perceived sufficiently by the participants (initial stimulus intensity), and the intensity of the stimulus in the target intervals was varied adaptively. The step size of the stimulus intensity initially corresponded to 4 dB and was reduced to 2 dB after two reversals and finally to 1 dB after four reversals. The mean of the last eight reversals in a block of 11 reversals was used as the hearing threshold estimate for that block.
2.2.2. Measurement of DLFs
The DLFs were measured when the bone-conduction stimuli were presented to the head (mastoid process), neck (sternocleidomastoid), and trunk (clavicle) to evaluate the frequency resolution of the distantly presented bone-conduction hearing.
As the stimuli, tone bursts with the CFs of 250, 500, 750, 1000, 2000, and 4000 Hz, including 30 ms rising/falling ramps, were used (duration: 400 ms).
The DLFs were measured using a two-up one-down two-alternative forced-choice adaptive procedure. The stimulus output levels were set to 15 dB SL for the mastoid process and sternocleidomastoid muscle and 10–15 dB SL for the clavicle.
In each trial, two tone bursts that were equally spaced in linear frequency on either side of the CF were presented, and the participants were requested to respond to the stimulus at a higher frequency. The DLF measurements were started from the deviation from the CF (Δf) at which the participants were able to discriminate between two stimuli sufficiently, and Δf was varied adaptively. The measurements were conducted until 11 reversals of the change in Δf were obtained, and the geometric mean of Δf/CF of the last eight reversals was used as the discrimination value.
2.2.3. Measurement of TMTFs
The TMTFs were measured when the bone-conduction stimuli were presented to the head (mastoid process), neck (sternocleidomastoid), and trunk (clavicle) to evaluate the temporal resolution of the distantly presented bone-conduction hearing.
The TMTF shows the threshold of sinusoidal amplitude modulation (SAM) detection as a function of the modulation frequency. The SAM detection threshold was determined systematically by measuring the modulation depth. A double sideband amplitude modulation was applied to 1000 Hz Hz and 4000 Hz sinusoidal carriers.
The SAM stimuli are expressed as follows:

Here,  is the amplitude of the entire stimulus,
is the amplitude of the entire stimulus,  is the modulation depth, and
is the modulation depth, and  and
and  are the modulation and carrier frequencies, respectively. The duration of the stimuli was 800 ms, which included 75 ms rising/falling ramps.
are the modulation and carrier frequencies, respectively. The duration of the stimuli was 800 ms, which included 75 ms rising/falling ramps.
The TMTFs were measured using a two-up one-down 3AFC adaptive procedure. The stimulus output levels were set to a level at which each participant was able to detect modulation sufficiently based on a 25 dB SL.
In each trial, three bone-conduction stimuli were presented sequentially. One of the three bone-conduction stimuli was modulated, whereas the others were unmodulated. The participants were requested to respond to the modulation interval. The TMTF measurements were started from the modulation depth  at which the modulation could be detected sufficiently by the participants, and the modulation depth in the modulation intervals was varied adaptively in the same manner as in the measurement of the hearing thresholds. The step size of the modulation depth initially corresponded to 4 dB (in units of 20 log) and was reduced to 2 dB after two reversals and finally to 1 dB after four reversals. The mean of the last eight reversals in a block of 11 reversals was used as the modulation threshold. The modulation frequencies were set to 10, 20, 50, 100, 125, 150, 175, and 200 Hz for the 1000 Hz carrier and 10, 20, 50, 100, 125, 150, 175, 200, 300, 400, 500, 600, 700, 800, 1000, and 1600 Hz for the 4000 Hz carrier, and the TMTF measurements were conducted for each modulation frequency.
at which the modulation could be detected sufficiently by the participants, and the modulation depth in the modulation intervals was varied adaptively in the same manner as in the measurement of the hearing thresholds. The step size of the modulation depth initially corresponded to 4 dB (in units of 20 log) and was reduced to 2 dB after two reversals and finally to 1 dB after four reversals. The mean of the last eight reversals in a block of 11 reversals was used as the modulation threshold. The modulation frequencies were set to 10, 20, 50, 100, 125, 150, 175, and 200 Hz for the 1000 Hz carrier and 10, 20, 50, 100, 125, 150, 175, 200, 300, 400, 500, 600, 700, 800, 1000, and 1600 Hz for the 4000 Hz carrier, and the TMTF measurements were conducted for each modulation frequency.
2.3. Measurement of TMTFs of air-conducted sounds as a function of the carrier level
In the current study, the intensities of the bone-conduction stimuli were lower (25 dB SL) than former studies 20,28) to prevent the perception of air-conducted emission from the vibrator. The TMTFs of the air-conducted sounds were measured as a function of the carrier level to examine the relationship between the TMTF and the stimulus intensity.
Four males (21–25 years) with no history of deficits in their hearing functions participated. The carrier and modulation frequencies were the same as those described in Sect. 2.2.3. The carrier levels were set to 15, 30, 45, 60, and 75 dB SL, and the stimuli were presented using a headphone (Sennheiser HD 660 S). The TMTFs were estimated for each participant in the same manner as described in Sect. 2.2.3.
3. Results
3.1. Insulation of air-conducted sounds
Figures 6(a) and 6(b) show the sound pressure level of the air-conducted sounds at the opening of the external auditory canal and the sound attenuation value by the earplugs and earmuff, respectively. The clavicle shows relatively larger sound pressure levels of approximately 50, 62, and 56 dB SPL, when a 2000, 3000, and 4000 Hz tone bursts were presented to the clavicle at 15 dB SL, respectively. However, the mastoid process and sternocleidomastoid shows sound pressure levels lower than 50 dB SPL. On the other hand, the sound attenuation values are larger than 43 dB at any frequency.
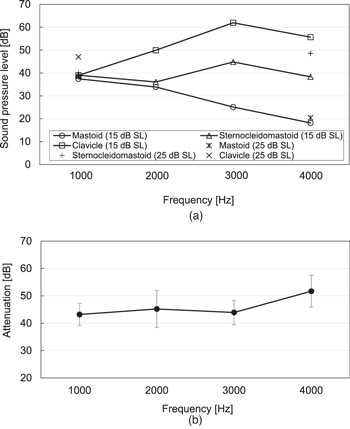
Fig. 6. Sound pressure level of air-conducted sounds at the opening of the ear canal and sound attenuation value measured to verify the insulating effect of the insulating method used in the experiments. (a) Sound pressure level of air-conducted sounds at the opening of the ear canal when bone-conduction stimuli were presented under the same conditions as the difference limen for frequency (DLF) and temporal modulation transfer function (TMTF) measurements. (b) Sound attenuation value of the insulating method used in the experiments. The data representation means ± standard deviation at each center frequency of the one-third octave band is applied to pink noise.
Download figure:
Standard image High-resolution image3.2. Hearing thresholds
Figure 7 shows the relative thresholds of the distantly presented bone-conducted sound with the hearing threshold for the mastoid process in each participant serving as the reference (0 dB). Although the hearing thresholds increased as the stimulus placements moved further away from the head, all the participants were able to perceive bone-conducted sounds even in the distal parts of the body. In the audible-frequency range, although the peak (approx. 5–10 dB) was observed at 500 Hz, the relative thresholds increased as the stimulus frequency increased, particularly at 1000–4000 Hz in the clavicle and acromion. On the other hand, in the ultrasonic range, the relative thresholds were lower than those in the audible-frequency range at all the stimulus placements.
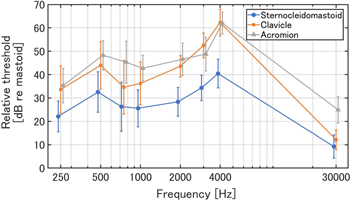
Fig. 7. (Color online) Relative threshold of the distantly-presented bone-conducted sound. The threshold for the mastoid process in each participant served as the reference (0 dB). The data represent means ± standard deviation at each stimulus frequency.
Download figure:
Standard image High-resolution imageThe two-way analysis of variance (ANOVA) of the stimulus placements and frequencies showed the significant main effects of these two variables, and a significant interaction between them (P < 0.05). The post-hoc test (Tukey HSD test) showed that the increases in the hearing thresholds relative to the mastoid process in the audible high-frequency range were significantly higher than those in the low-frequency range (sternocleidomastoid: 250, 500, 750, and 1000–4000 Hz, clavicle: 250, 500, 750, and 1000–3000 Hz and 250, 500, 750, and 1000–4000 Hz, acromion: 250–3000 Hz and 250, 500, and 750–4000 Hz). In the clavicle and acromion, those in the high-frequency range were significantly higher than those in the middle-frequency range (clavicle: 2000–4000 Hz, acromion: 2000 and 3000–4000 Hz). Moreover, those in the ultrasonic range (30000 Hz) were significantly lower than those in the audible-frequency range (250–4000 Hz). In the ultrasonic range, the relative threshold increased significantly at the acromion compared with the other locations, whereas in the audible-frequency range, the relative threshold decreased significantly at the sternocleidomastoid muscle compared with the other locations.
3.3. DLFs
Figure 8 shows the DLFs at each stimulus placement. All the participants were able to discriminate the frequency at all the stimulus placements and CFs. Generally, the DLFs were approximately 0.3% at all the CFs at the mastoid process and sternocleidomastoid muscle. In the clavicle, the DLF was equivalent to that of the mastoid process and sternocleidomastoid muscle at 500–2000 Hz, whereas it was higher at 250 and 4000 Hz. The two-way ANOVA of the stimulus placements and CFs showed the significant main effects of these two variables, and a significant interaction between them (P < 0.05). The post-hoc test (Tukey HSD test) showed that the DLF increased significantly at 250 and 4000 Hz in comparison with that at the other frequency ranges in the clavicle.
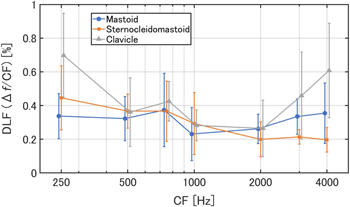
Fig. 8. (Color online) Difference limens for frequency (DLFs) expressed as a proportion of the center frequency (CF) for each stimulus placement. 25) The data represent means ± standard deviation at each CF.
Download figure:
Standard image High-resolution image3.4. TMTFs of bone-conducted sounds
Figures 9(a) and 9(b) show the modulation thresholds of the bone-conducted sounds at each stimulus placement using the 1000 Hz and 4000 Hz sinusoidal carriers, respectively. In the case of the 1000 Hz carrier, no significant variation depending on the increase in the modulation frequency was observed at any of the stimulus placements. Additionally, no significant increase was observed as the stimulus placements moved further away from the head. In the case of the 4000 Hz carrier, the modulation thresholds increased at a modulation frequency of 100 Hz or higher. In the modulation frequency range, although the modulation thresholds of the mastoid process were higher than those of the sternocleidomastoid muscle, no significant difference was observed.
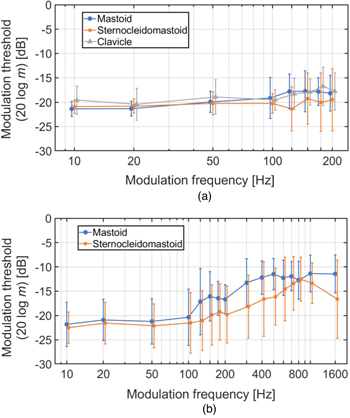
Fig. 9. (Color online) Modulation-detection thresholds of bone-conducted sound in the audible-frequency range at the carrier frequencies of (a) 1000 Hz and (b) 4000 Hz. 25) The data represent means ± standard deviation at each modulation frequency.
Download figure:
Standard image High-resolution image3.5. TMTFs of air-conducted sounds as a function of the carrier level
Figures 10(a) and 10(b) show the modulation thresholds of the air-conducted sounds at each carrier level using the 1000 Hz and 4000 Hz sinusoidal carriers, respectively. At high carrier levels, the modulation thresholds decreased above a modulation frequency of 100 Hz for the case of the 1000 Hz carrier and 400 Hz for the case of the 4000 Hz carrier, whereas the shapes of the TMTFs were similar to those of the bone-conducted sounds obtained in this study at low carrier levels.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Fig. 10. (Color online) Modulation-detection thresholds of air-conducted sound at different carrier levels at the carrier frequencies of (a) 1000 Hz and (b) 4000 Hz. The data representation means ± standard deviation at each modulation frequency.
Download figure:
Standard image High-resolution image{kind=link}
4. Discussion
4.1. Insulation of air-conducted sounds
When a 3000 Hz tone burst was presented to the clavicle at 15 dB SL, the sound pressure level was the highest at approximately 62 dB SPL. On the other hand, the sound attenuation value at 3000 Hz was approximately 44 dB. In this case, it is considered that the air-conducted sound entering the external auditory canal was perceived as a low loudness sound of about 10 dB SL because the absolute threshold of human hearing at 3000 Hz is approximately 8 dB SPL. 29) Therefore, we need to consider that air-conducted sound may affect the threshold at 3000 Hz on the clavicle, however, it seems that the radiation of air-conducted sounds from the vibrator does not produce significant changes on the current results.
At 2000 Hz, the sound pressure levels were approximately 34–50 dB SPL, whereas the sound attenuation value was approximately 45 dB. So, it is considered that the amount of air-conducted sound sufficient to be perceived by the participants did not enter the external auditory canal because the absolute threshold at 2000 Hz is equivalent to that at 3000 Hz. 29) The same is true for the other frequency ranges, except for 3000 Hz. These results indicate that the air-conducted sounds were sufficiently insulated using the urethane and silicone earplugs and earmuff to evaluate only the perception of bone conduction.
4.2. Hearing thresholds
The bone-conducted sounds presented to the distal parts of the body were perceived in all the vibrator locations by all the participants. This result suggests the possibility of developing a novel bone-conduction device using "distant presentation." The hearing thresholds increased as the stimulus placements moved further away from the head, as in our previous study. 24) On the other hand, a dip in the hearing threshold of approximately 5–10 dB at 1000 Hz, shown in the previous study, was not observed. This discrepancy in the hearing threshold might be caused by a difference in the vibrator (previous study: RadioEar B-71) or the method of holding the vibrator; however, further studies are required to elucidate the detailed mechanism.
In this study, the increase in the hearing threshold from the mastoid process in the audible-frequency range was approximately 20–40 dB in the sternocleidomastoid muscle, and 35–65 dB in the clavicle and acromion, which are larger than those in the ultrasonic range. In addition, our previous study on the hearing threshold of distantly presented BCU has shown that the increase in the hearing threshold was only 20 dB in the upper arm and 27 dB in the lower arm. 20) These results indicate that the distance attenuation of bone-conducted sound in the human body is much larger in the audible-frequency range than that in the ultrasonic range. Furthermore, in the ultrasonic range, significant differences in the relative threshold between the clavicle and the acromion, which are at equivalent distances from the head, were observed, whereas no significant difference was observed in the audible-frequency range. This result suggests that the BCU perception is affected not only by the propagation distance but also by other factors, such as the differences in the biological tissue present in the propagation process. On the other hand, the perception of distantly presented bone-conducted sound in the audible-frequency range is strongly dependent on the propagation distance.
4.3. DLFs
At the mastoid process and sternocleidomastoid muscle, the DLF was approximately 0.3% for all the CFs, which was the same as that of the air-conducted sound. 28,30–32) This result indicates that the frequency resolution of distantly presented bone-conduction hearing is equivalent to that of air-conducted sound when bone-conducted sound is presented to a body part relatively close to the head. In addition, no significant difference was observed in the DLF among stimulus placements for almost all the CFs, whereas the hearing thresholds increased as the stimulus placements moved further away from the head. These results indicate that the degradation of frequency information that occurs during the propagation process of bone-conducted sounds is small.
4.4. TMTFs
No significant difference among stimulus placements was observed at any of the modulation frequencies, regardless of the carrier frequency, when bone-conducted sound was presented to the distal parts of the body. This result indicates that no degradation of the temporal information of bone-conducted sounds occurs during the propagation process in the human body.
According to a previous study on the TMTF of air-conducted sound, 33) the sidebands caused by amplitude modulation were perceived as another pitch above a certain modulation frequency, and the modulation threshold subsequently decreased. In contrast, in this study, no significant decrease in the modulation threshold of bone-conducted sound was observed as the modulation frequency increased. Moreover, it was confirmed that the shapes of the TMTFs of the air-conducted sounds were different from those of the bone-conducted sounds obtained in this study at high carrier levels, whereas they were similar at low carrier levels. These results indicate that the difference between the TMTF of bone-conducted sound obtained in this study and that of air-conducted sound obtained in the previous study occurred because no significant sideband exceeding the level of the noise floor was caused because the stimulus intensity was set to a smaller level (25 dB SL) to prevent the perception of air-conducted sounds radiated from the vibrator. Therefore, it is necessary to consider a more effective insulation method for air-conducted sounds and a method to eliminate the effect of vibratory sensation, which may be generated due to the increase in stimulus intensity, to elucidate the detailed perceptual mechanisms of distantly presented bone-conducted sound in the audible-frequency range.
5. Conclusions
In this study, to examine the basic perceptual characteristics of distantly presented bone-conducted sound in the audible-frequency range, hearing thresholds, DLFs, and TMTFs were measured under the condition that air-conducted sounds were insulated. The results obtained indicated that bone-conducted sound can be perceived at the distal parts of the body, even in the audible-frequency range, whereas the distance attenuation is larger than that in the ultrasonic range. Moreover, the degradation of frequency and temporal information that occurred in the propagation process of bone-conducted sounds was sufficiently small for the transmission of sound information. These results provide useful information not only for elucidating the mechanisms of the perception and propagation of distantly presented bone-conducted sound but also for developing novel bone-conduction devices using "distant presentation" that can transmit the sound information selectively to users who touch the device.
Acknowledgments
This study was supported by JSPS KAKENHI Grant Numbers 19K22950 and 20H04497 and a research grant for the Next Generation Research Incubator from the Institute for Global Prominent Research, Chiba University for SN.