

Abstract
Low birth weight is a leading cause of childhood morbidity and mortality globally, especially in low- and middle-income countries. Individual trace element exposure during pregnancy is associated with birth weight; however, information on potential mixture effects of multiple-elements exposure on birth weight are limited. In this study, we assessed the effects of single element and element mixtures on birth weight among 745 mother-infant pairs from a prospective birth cohort established in Bangladesh from 2008 to 2011. Using inductively coupled plasma mass spectrometry, we measured 56 elements in cord blood collected at delivery. Multivariate linear regression was used to evaluate the individual effect of element exposure on birth weight. Then, we also applied regression model based on categorical variables according the interquartile range (IQR) and restricted cubic spline to explore potential non-linear associations. Bayesian kernel machine regression (BKMR) and weighted quantile sum (WQS) regression were used to assess the mixture effects on birth weight. We found significant negative associations between exposure to lithium (Li), manganese (Mn), cobalt (Co), copper (Cu), yttrium (Y), and erbium (Er) and birth weight, while the concentration of selenium (Se) was positively associated with birth weight. Li was identified as the most important predictor of birth weight by WQS regression and cumulative exposure to element mixtures (Li, Mn, Cu, Co, Y, and Er) was associated with decreased birth weight, birth weight decreasing by 64.73 g with per each unit increment of the element risk score (ERS) based on WQS. Interestingly, the presence of Se during pregnancy may attenuate the risk of low birth weight by its main protective and antagonistic effects against toxic elements.
Export citation and abstract BibTeX RIS

Original content from this work may be used under the terms of the Creative Commons Attribution 4.0 licence. Any further distribution of this work must maintain attribution to the author(s) and the title of the work, journal citation and DOI.
Abbreviations
| BMI | body mass index |
| CV | coefficient of variation |
| FDR | false discovery rate |
| ICP-MS | inductively coupled plasma mass spectrometry |
| LOD | limit of detection |
| OR | odds ratio |
| 7Li | lithium |
| 9Be | beryllium |
| 11B | boron |
| 23Na | sodium |
| 24Mg | magnesium |
| 27Al | aluminum |
| 39K | potassium |
| 44Ca | calcium |
| 45Sc | scandium |
| 47Ti | thallium |
| 51V | vanadium |
| 52Cr | chromium |
| 55Mn | manganese |
| 56Fe | iron |
| 59Co | cobalt |
| 60Ni | nickel |
| 63Cu | copper |
| 66Zn | zinc |
| 71Ga | gallium |
| 75As | arsenic |
| 78Se | selenium |
| 85Rb | rubidium |
| 88Sr | strontium |
| 89Y | yttrium |
| 90Zr | zirconium |
| 93Nb | niobium |
| 95Mo | molybdenum |
| 107Ag | silver |
| 111Cd | cadmium |
| 118Sn | stannum |
| 121Sb | antimony |
| 133Cs | caesium |
| 137Ba | barium |
| 139La | lanthanum |
| 140Ce | cerium |
| 141Pr | praseodymium |
| 146Nd | neodymium |
| 147Sm | samarium |
| 151Eu | europium |
| 157Gd | gadolinium |
| 159Tb | terbium |
| 163Dy | dysprosium |
| 165Ho | holmium |
| 166Er | erbium |
| 169Tm | thulium |
| 172Yb | ytterbium |
| 175Lu | lutetium |
| 178Hf | hafnium |
| 181Ta | tantalum |
| 182W | wolfram |
| 202Hg | hydrargyrum |
| 205Tl | thallium |
| 208Pb | lead |
| 209Bi | bismuth |
| 232Th | thorium |
| 238U | uranium |
| 95% CI | 95% confidence interval |
| REE | rare earth elements |
| Bayesian kernel machine regression | (BKMR) |
| WQS | weighted quantile sum |
| ERS | elements risk score. |
Introduction
Birth weight is an important gauge of fetal health and a determinant of perinatal, neonatal, and infant mortality and morbidity [1]. Every year, an estimated 20 million (15.5%) infants are born with low birth weight (<2500 g) globally and approximately 95.6% of these births occur in low- and middle-income countries [2, 3]. Infants with low birth weight are approximately 20 times more likely to die during infancy and childhood than babies born at normal birth weight [2]. Low birth weight remains a leading public health problem, especially in developing nations.
Studies have shown that prenatal exposure to trace elements, occurring widely and naturally in environment, can disrupt fetal growth and functions of organ systems. Elements, such as lead (Pb), are toxicants to the development of fetus, even if present at low concentrations [4, 5]. On the hand, some elements are essential for fetal growth, including iron (Fe), magnesium (Mg), molybdenum (Mo), selenium (Se), and zinc (Zn). And, some essential nutrient elements can attenuate the toxicity of some element exposure [6, 7]. For example, Se supplementation may decrease serum copper (Cu) levels and might provide protection against Ni toxicity in low-birth-weight, premature infants [8, 9]. However, excess or insufficient levels of these required elements may both increase the risk of low birth weight [10]. However, There is little known about the potential health effects of simultaneous exposure to various elements and element mixtures on low birth weight [11].
The transfers of exposure from mother to fetus have mainly through umbilical cord blood or red blood cells and umbilical cord blood can reflect elements exposure during the period of intrauterine life [12, 13].Thus umbilical cord serum can be used to indicate prenatal exposure to a variety of elements, which is easily available at delivery [14]. Moreover, the concentrations of trace elements in serum do not need to be calibrated, making it easy to analyze [15]. This study was designed to identify the landscape of elements in cord serum and examine the possible effects of element exposure on birth weight based on a prospective birth cohort established in rural Bangladesh. Further, Bayesian kernel machine regression (BKMR) and weighted quantile sum regression (WQS) were used to assess the associations between element mixtures and birth weight.
Methods
Study population
We conducted a prospective cohort study to identify associations between elements exposure and birth outcomes from 2008 to 2011 at Sirajdikhan and Pahna Sadar Upazilas in Bangladesh. The following study population inclusion criteria were used: (1) an ultrasound confirming a singleton pregnancy of ≤16 weeks gestation, (2) tube well water as the primary drinking water source for at least 6 months before enrollment, and (3) prenatal care provided by Dhaka Community Hospital Trust (DCH) throughout pregnancy and birth. Cohort recruitment and enrollment processes and other study details have been described [16]. The study was described in detail to all participants, and informed consent was obtained before study enrollment. All protocols performed in studies involving human participants were reviewed and approved by the Human Research Committees at Harvard T.H. Chan School of Public Health, Nanjing Medical University, and DCH.
In all, 1,613 eligible individuals were recruited at enrollment, of which 244 (15.2%) experienced fetal loss or neonatal death, and 302 families (18.8%) were lost to follow-up because of family migration or study withdrawal. At delivery, there were 745 mother-infant pairs with umbilical cord serum samples available.
Outcome and covariates
Birth weight was measured within 120 min of delivery on a pediatric scale calibrated and rounded to the nearest 10 g before each measurement by trained healthcare workers. Gestational age was determined through ultrasonography by a licensed general practitioner using either (1) the gestational sac mean diameter if the pregnancy was between 4 and 7 weeks or (2) the crown–rump length if the pregnancy was between 7 and 16 weeks.
Demographic and anthropometric information of mothers and children were collected at less than 16 weeks gestation and birth. Other covariates in this analysis were collected at the time of enrollment using a structured questionnaire, including maternal age, body mass index (BMI), age of marriage, maternal and spouse education level, family income level, and second-hand smoking exposure.
Materials
Umbilical cord serum samples were collected immediately at delivery. Cord serum samples from newborns were obtained through venous puncture of the umbilical cord. All samples were collected and kept at −80 °C, shipped to the Trace Metals Laboratory at the Harvard Chan School, received in perfect condition, and correctly identified.
We analyzed 56 elements in umbilical cord serum (Figure S1 (available online at stacks.iop.org/ERC/3/105001/mmedia)) using an ICAP QC inductively coupled plasma mass spectrometer (ICP-MS) (Agilent 7700x ICP-MS, USA) at Shanghai Biotree Biotech Co., Ltd, including 9 alkali or alkaline earth metals [beryllium (9Be), sodium (23Na), magnesium (24Mg), potassium (39K), calcium (44Ca), rubidium (85Rb), strontium (86Sr), caesium (133Cs), and barium (137Ba)], 10 transition metals [thallium (47Ti), vanadium (51V), chromium (52Cr), manganum (55Mn), iron (56Fe), cobalt (59Co), nickel (60Ni), copper (65Cu), zinc (66Zn), and antimony (121Sb)], 16 rare earth elements (REEs) [scandium (45Sc), yttrium (89Y), lanthanum (139La), cerium (140Ce), praseodymium (141Pr), neodymium (146Nd), samarium (147Sm), europium (151Eu), gadolinium (157Gd), terbium (159Tb), dysprosium (163Dy), holmium (165Ho), erbium (166Er), thulium (169Tm), ytterbium (172Yb), and lutetium (175Lu)], and 21 other elements [lithium (7Li), boron (11B), aluminum (27Al), gallium (71Ga), arsenic (75As), selenium (78Se), zirconium (90Zr), niobium (93Nb), molybdenum (95Mo), silver (107Ag), cadmium (111Cd), stannum (118Sn), hafnium (178Hf), tantalum (181Ta), wolfram (182W), hydrargyrum (202Hg), thallium (205Tl), lead (208Pb), bismuth (209Bi), thorium (232Th), and uranium (238U)].
For elements analyses, we followed a validated procedure for human blood with certified reference materials. Briefly, 60 μl of cord blood were diluted using 1800 μl of ammonia solution (1% of NH4OH), and internal standards (ISTD) were added. The ISTD solution comprised Li (40 μg l−1) and rhodium (Rh), indium (In), and rhenium (Re) (20 μg l−1 each). A blank sample was also introduced to each of the 10 samples to ensure that there was no memory effect for any element. The limits of detection (LOD) and limits of quality (LOQ) were established as the signals that were three and ten times higher, respectively, than the signal of the average of ten consecutive blank measurements. Element concentrations below the LOD were imputed by LOD/2.
Statistical analyses
Descriptive statistics [relative standard deviation (RSD), median] of umbilical cord blood concentrations were calculated to describe the distributions of element concentrations among study participants. All concentrations of elements displayed skewed distributions (Figure S1) and thus were natural log transformed before statistical analysis.
Multivariate linear regression
Multivariate linear regression was used to evaluate the associations between individual element exposure measured in cord blood and birth weight adjusted for covariates, including maternal age, gestational age, infant sex, BMI, second-hand smoking, marriage age, education level, and family income levels, which were significantly associated with the outcome (P ≤ 0.05). To evaluate potential non-linear associations, linear models were run with each element exposure converted as a categorical variable based on interquartile range (IQR). We also explored associations between elements and birth weight stratified by population characteristics. Statistical significance was evaluated with the false discovery rate (FDR) to control for multiple comparisons, and an FDR-q ≤ 0.05 was considered statistically significant.
Bayesian kernel machine regression (BKMR)
To explore interaction effects between multiple metals on birth weight, we used Bayesian kernel machine regression (BKMR), a non-parametric Bayesian variable selection framework for conducting mixture analysis without the assumption of linearity of the associations [17]. BKMR combines Bayesian and statistical learning methods to regress an exposure–response function iteratively by a Gaussian kernel function. BKMR can identify interactions between element mixtures. Here, BKMR modeled flexible function of element concentrations while adjusting for the same covariates described above. We assessed bivariate exposure-response effects of two metals if the second metal was fixed at the 10th, 50th, or 90th quantile while the other element was at the median.
Assessment of interaction effects
We further verified the interaction effects among identified trace elements by BKMR using linear regression models with cross-product terms and assessed the significance of the coefficients using the Wald statistic. Further, categorical variables and restricted cubic spline were applied to explore metal-metal non-linearity interaction effects. For the categorical approach, levels of identified elements were re-categorized as 'low' (1st and 2nd tertiles) and 'high' (the 3rd tertile) [8]. For example, we analyzed effects as low Li with high Er, low Li with low Er, high Li with high Er, and high Li with low Er. Also, we added interaction effects in the restricted cubic spline model to explore the potential non-linear interaction effects between elements by setting the target elements at different quantiles [18]. And, FDR was used to evaluate statistical significance to control for multiple comparisons.
Weighted quantile sum (WQS) regression
Weighted quantile sum (WQS) regression analyses were applied to construct an element risk score (ERS) adjusting for the same covariates described above. WQS regression was developed to assess the combined and discrete effects of multiple predictors in the context of correlated high-dimensional mixtures, which estimates an index that identifies the influential exposure variables with non-negligible weights and tests for associations between the exposure index and an outcome in a traditional linear framework as: g(μ) = β0 + β1WQS + z'ϕ. Here, g(μ) reflects a nonlinear link function allowing generalization to continuous, binary, and other distributions. As in typical regression approaches, β0 represents the model intercept while β1 represents the parameter estimate for the co-exposure index, represented here as WQS; the significance of this parameter reflects a straightforward test of associations between the co-exposure index and the outcome. The WQS index is constructed such that  where
where  indicates a vector of empirically estimated weights for each mixture component, and
indicates a vector of empirically estimated weights for each mixture component, and  indicates the values of the mixture variables to each subject per element, which have been standardized [19].
indicates the values of the mixture variables to each subject per element, which have been standardized [19].
All statistical analyses were performed using R version 3.6.0.
Results
Characteristics of the study population and trace elements
Demographic characteristics of the 745 mother-infant pairs and associations between demographic characteristics and birth weight are presented in table 1. The mean marriage age of the study population was 17.58 ± 2.29 years, with 59.46% of women married before 18 years of age. Further, 62.55% of women had a normal pre-pregnancy BMI (18.5–23.9 kg m−2), with a mean weight of 46.73 ± 7.74 kg and height of 151.09 ± 5.66 cm. In addition, 312 (41.88%) women were exposed to second-hand smoking, 188 (25.23%) spouses had no formal education, 245 (32.89%) had secondary education, and 320 (42.95%) received an income between 4000 and 6000 taka. Among infants, the average birth weight was 2841.05 g (standard deviation: 424.09 g; range: 800–4500 g), 376 (50.47%) were boys, 159 (21%) infants were born preterm (< 37 weeks of gestation), and 137 (18.39%) were small for gestational age.
Table 1. Characteristics of study participants and association with birth weight (g).
| Statistics | b (95% CI) | P value | |
|---|---|---|---|
| Baseline age (years) | 22.83 ± 4.10 | −0.723 (−8.163, 6.718) | 0.849 |
| Marriage age (years) | 17.58 ± 2.29 | 22.237 (9, 35.474) | 0.001 |
| <18 years | 443 (59.46) | Reference | |
| ≥18 years | 302 (40.54) | 69.753 (7.886, 131.62) | 0.027 |
| BMI (kg m−2) | 20.47 ± 3.20 | 21.065 (11.664, 30.467) | <0.001 |
| <18.5 | 212 (28.46) | Reference | |
| 18.5–24.9 | 466 (62.55) | 77.196 (8.865, 145.528) | 0.027 |
| >24.9 | 67 (8.99) | 211.647 (96.045, 327.249) | <0.001 |
| Weight (kg) | 46.73 ± 7.74 | 11.597 (7.744, 15.450) | <0.001 |
| Height (cm) | 151.09 ± 5.66 | 10.27 (4.933, 15.608) | <0.001 |
| Gestational age (weeks) | 37.98 ± 2.07 | 92.703 (79.550, 105.856) | <0.001 |
| ≥37 weeks | 586 (78.66) | Reference | |
| <37 weeks | 159 (21.34) | −452.054 (−518.952, −385.156) | <0.001 |
| Second-hand smoking | |||
| No | 433 (58.12) | Reference | |
| Yes | 312 (41.88) | −99.299 (−160.654, −37.945) | 0.002 |
| Education | |||
| No formal | 108 (14.50) | Reference | |
| Primary | 245 (32.89) | 176.454 (81.441, 271.466) | <0.001 |
| Secondary or higher | 392 (52.62) | 187.341 (97.946, 276.737) | <0.001 |
| Education Spouse | |||
| No formal | 188 (25.23) | Reference | |
| Primary | 247 (33.15) | 89.018 (9.058, 168.979) | 0.029 |
| Secondary or higher | 310 (41.61) | 129.855 (53.487, 206.223) | <0.001 |
| Income | |||
| ≤4000 | 333 (44.70) | Reference | |
| 4001–6000 | 320 (42.95) | 3.836 (−60.873, 68.544) | 0.908 |
| >6000 | 87 (11.68) | 164.524 (64.996, 264.052) | 0.001 |
| Birth length | 46.43 ± 2.81 | 47.075 (36.744, 57.405) | <0.001 |
| Birth head circumference | 32.65 ± 1.31 | 124.221 (102.763, 145.68) | <0.001 |
| Number of pregnancies | |||
| 0 | 313 (42.01) | Reference | |
| 1 | 230 (30.87) | 33.48 (−38.61, 105.56) | 0.363 |
| >1 | 202 (27.11) | −49.81 (−124.72, 25.1) | 0.193 |
| Sex | |||
| Boy | 376 (50.47) | Reference | |
| Girl | 369 (49.53) | −86.001(−146.638, −25.365) | 0.006 |
| Birth place | |||
| Home | 387 (51.95) | Reference | |
| Clinic | 46 (6.17) | 256.009 (130.131, 381.888) | <0.001 |
| Hospital | 309 (41.48) | 202.609 (141.032, 264.185) | <0.001 |
| Birth type | |||
| Vaginal | 465 (62.42) | Reference | |
| Cesarean | 280 (37.58) | 189.894 (128.474, 251.314) | <0.001 |
Note: continuous variables are presented as mean ± standard deviation; categorical variables are presented as frequency and proportion [n (%)]; b (95% CI) represents the coefficient and confidence interval of the association between the variable and birth weight.
Descriptive statistics (LOD, LOQ, RSD, and quartiles) of cord serum element concentrations are presented in table S1. Most of the samples had detectable element concentrations; only three elements exhibited concentrations higher than LOD in less than 50% of samples and were excluded from the subsequent statistical analysis [Cd (56.387% > LOD), Lu (70.47% > LOD), and Tl (69.66% > LOD)]. All the elements followed right-skewed distributions (Figure S1).
Associations between individual element and birth weight
Multivariate linear regression model for each element adjusted for common covariates identified seven elements related to birth weight (FDR-q ≤ 0.05) (figure 1(A) and table S2). The presence of Li [b = −33.5, 95% CI: (−46.26, −20.44), P = 5.21 × 10−7, FDR-q = 3.07 × 10−5)], Mn [b = −38.94, 95% CI: (−63.24, −14.64), P = 0.002, FDR-q = 0.021], Co [b = −49.68, 95% CI: (−73.01, −26.35), P = 3.37 × 10−5, FDR-q = 0.001], and Cu [b = −74.89, 95% CI: (−121.52, −28.27), P = 0.002, FDR-q = 0.021] in umbilical cord serum were associated with low birth weight respectively. Also, we found the concentration of Y [b = −45.57, 95% CI: (−76.52, −14.62), P = 0.004, FDR-q = 0.039] and Er [b = −41.33, 95% CI: (−69.82, −12.84), P = 0.005, FDR-q = 0.039], both REEs, were associated with decreased birth weight. Interestingly, per each unit increment of Se umbilical cord serum levels was associated with an average increase in birth weight of 161.77 g [95% CI: (83.98, 239.56), P = 5.10 × 10−5, FDR-q = 0.001]. The relationships between above elements and birth weight according to quartiles of exposure were shown in table S3. And the results of categorical analyses shown that exposure to higher concentrations of elements would have greater effects on birth weight. Significant correlations between the above identified elements are shown in figure 1(B).
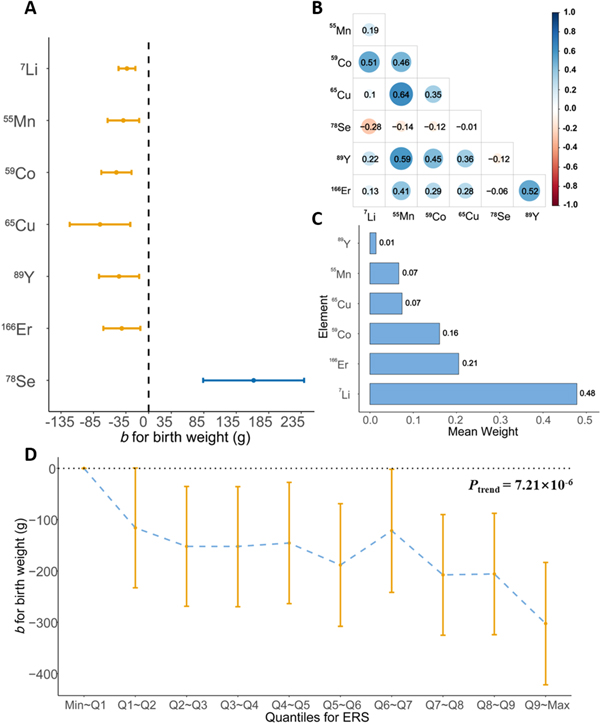
Figure 1. Effect estimates for increase in loge transformed exposure and element risk score on birth weight. (A) Multiple linear models were adjusted for maternal age, gestational age, sex, BMI, second-hand smoking, marriage age, education level, and income level to assess for the association between individual element exposure and birth weight. (B) Correlations between Li, Co, Cu, Se, Y, and Er. (C) The mean weight for the effect of element mixtures (Li, Mn, Co, Cu, Y, and Er) on birth weight estimated by weight quantile sum (WQS) regression. (D) Visualization using a quantile plot provided an illustration of the effect of increasing element risk score (ERS) on birth weight.
Download figure:
Standard image High-resolution imageAlso, the associations between these elements and birth weight stratified by population characteristics were generally consistent with our findings (Table S4). Interestingly, the negative effects of Mn and Cu seemed to be more obvious in preterm birth. Pregnant women exposed to second hand smoking or marrying before 18 years may be affected easily by elements exposure.
Element mixture analyses
BKMR analyses were used to explore potential interactions among candidate elements, indicating potential interactive associations between Li and other elements (Mn, Co, Cu, Se, Y, and Er) (figure 2). We also further explored the protective effect of Se against toxicity of the other elements on birth weight.
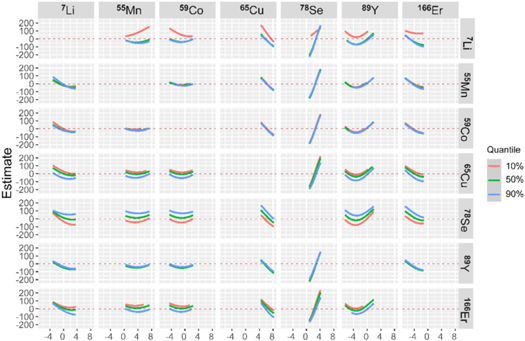
Figure 2. Bivariate predictor-response function for the effect of mixtures on birth weight estimated by BKMR. Bivariate exposure-response functions for interaction or joint effects of element mixtures (Li, Mn, Co, Cu, Se, Y, and Er) on birth weight estimated by Bayesian kernel machine regression (BKMR); for example, Er when Li is fixed at either the 10th, 50th, or 90th percentile and the other elements are fixed at the median (bottom left panel). The model was adjusted for maternal age, gestational age, sex, BMI, second-hand smoking, marriage age, education level, and income level.
Download figure:
Standard image High-resolution imageMultivariate linear regression showed that there was no significant interaction on the multiplicative scales after multiple testing correction (FDR-q > 0.05) (Table S5). Metal-metal non-linearity interaction analyses showed that high Li exposure weakened the protectiveness of Se and aggravated the toxicity of other elements exposure on birth weight (Table S6). For example, there was a significant negative association between element exposure and birth weight only among those exposed to high levels of Er and Li compared with the other three groups. By contrast, the negative effect of element exposure on birth weight could be weakened in the population with high Se concentration compared with those with low Se concentration (Table S7).
Restricted cubic spline showed that associations between the identified elements (except Li) and birth weight differed by varying the series quantiles of Li and exposure to high Li may increase the risk of lower birth weight (figure 3). For example, Er had a strengthened negative association on birth weight according to the increased percentile of Li concentration (figure 3(F)), while the toxicity of Er on birth weight was considerably weakened with the increased percentile of Se concentration (figure 4(F)). High concentration of Se could weaken negative effects of toxicity elements exposure and similar opposite patterns of other non-linear interactions to Li between Se and the other risk elements are shown in figure 4.
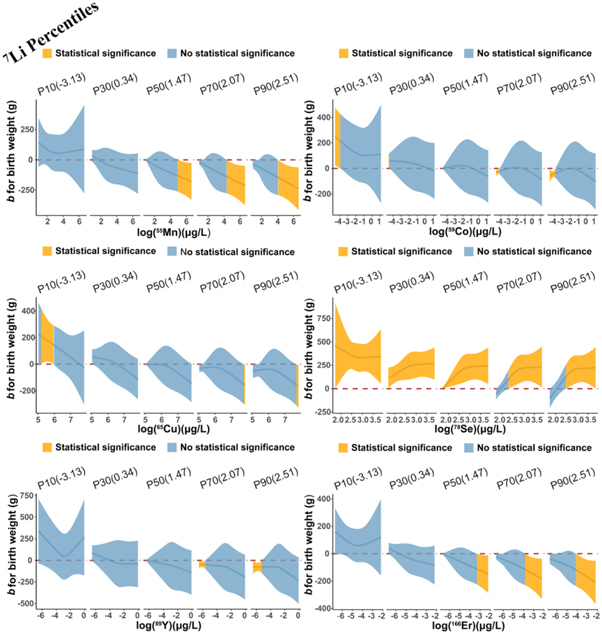
Figure 3. Toxic effect of elements on birth weight as modified by Li. The restricted cubic spline for the relationships between identified elements and birth weight in different quantiles of loge Li level [−3.13 μg l−1 (10%), 0.34 μg l−1 (30%), 1.47 μg l−1 (50%), 2.07 μg l−1 (70%), 2.51 μg l−1 (90%)]. Lines represent coefficients based on restricted cubic splines for the log-transformed levels of elements in the linear model. Adjustment factors included maternal age, gestational age, sex, BMI, second-hand smoking, marriage age, education level, and income level.
Download figure:
Standard image High-resolution image
{kind=link}
{kind=link}
{kind=link}
Figure 4. Toxic effect of elements on birth weight as modified by Se. The restricted cubic spline for the relationships between identified elements and birth weight in different quantiles of loge Se level [2.28 μg l−1 (10%), 2.55 μg l−1 (30%), 2.76 μg l−1 (50%), 2.91 μg l−1 (70%), 3.19 μg l−1 (90%)]. Lines represent coefficients based on restricted cubic splines for the log-transformed levels of elements in the linear model. Adjustment factors included gestational maternal age, gestational age, sex, BMI, second-hand smoking, marriage age, education level, and income level.
Download figure:
Standard image High-resolution image{kind=link}
Using the WQS model, the six risk elements (Li, Mn, Co, Cu, Y, and Er) were spontaneously evaluated for their joint effect. The ERS was constructed as a weighted sum of the elements using the mean weight of elements from the WQS regression attributed to the mean contributions of Li (48%), Er (21%), Co (16%), Cu (7%), Mn (7%), and Y (1%) (figure 1(C)). The ERS ranged from −3.10 to 2.21 with a mean (SD) of −0.3 (1.20). Note that the higher ERS index meant higher risk element exposure because WQS regression focuses inference in the negative direction in this study. Higher ERS values indicated more susceptibility to decreased birth weight in relation to cumulative exposure to element mixtures; per each unit increment of ERS, birth weight decreased 64.73 g [95% CI: (−86.75, −42.71), P = 1.23 × 10−8] after adjustment for the same covariates above. Further, the quantile analyses illustrated that the negative effect of element mixture on birth weight was more obvious among those with a high ERS [b = −21.73, 95% CI: (−31.16, −12.31), Ptrend = 7.21 × 10−6] (figure 1(D) and table S8).
Discussion
In this study, we described 56 elements measured in cord serum blood and assessed effects of exposure to individual element and mixtures on birth weight. Multivariate linear regression demonstrated that concentrations of Li, Mn, Co, Cu, Y, and Er in cord serum were negatively associated with birth weight and confirmed the protective effect of Se. BMKR analyses suggested potential interactions between Li and other identified elements, and WQS identified Li as the most important predictor of birth weight. ERS constructed based on the WQS illustrated that cumulative exposure to element mixture (Li, Mn, Cu, Co, Y, and Er) is associated with more decreased birth weight. Interestingly, our results indicated that Se could attenuate and antagonize the toxicity of elements on birth weight. Our findings highlight the importance of assessing the effects of single and element mixtures on birth weight.
Li has been an effective treatment for relapse prevention in bipolar spectrum disorder during pregnancy and postpartum [20]. However, Li has a narrow therapeutic range from 0.5 to 1.2 mmol l−1 and higher levels may lead to toxicity [21], which has been classified as a teratogenic substance by the U.S. Food and Drug Administration [22]. What's more, it has been reported that Li exposure would increase risks of impaired fetal size [22]. In this study, we found that Li was a key exposure inversely associated with birth weight. Previous studies have found that exposure to Li during pregnancy would increase the risk of adverse birth outcome, such as miscarriage, prematurity, fetal goiter, hypothyroidism, and low birth weight [23, 24]. Drinking water may be the main source of Li in Bangladesh, which is a common and general source and can easily cross the placenta to the fetus [25, 26].
Insufficient and excess essential element concentrations could both affect fetal growth [27–29]. Here, we found that essential nutrients such as Mn, Cu, and Co decreased birth weight, all of which are also cofactors of the major antioxidant enzymes. Mn, which is present in air, soil, and water, is vital for optimal fetal growth and development [30]. Previous studies found that the association between Mn and birth weight follows an inverse 'U-shaped' curve [31–33]. In this study, the concentration of Mn (median: 10.15 μg l−1 (range: 5.62–789.51 μg l−1)) was higher than in other studies and well above the safe level in cord serum 5.0 μg l−1 [33–35]. The negative effect of Mn on birth weight in our research indicated the overexposure in Bangladesh. Mn may affect birth weight through certain matrix metalloproteinases, markers for inflammatory and oxidative stress [36].
Cu deficiency or overexposure are both associated with adverse birth outcomes and previous study has demonstrated that Cu may be an important factor triggering the condition of low birth weight [37, 38]. Appropriate concentrations of Cu for infant development and a possible 'safe level' remain unknown. However, it has been reported that the average umbilical cord blood or serum Cu concentrations were between 220 and 520 μg l−1 in before epidemiologic studies [37, 39, 40] , which were much lower than our study results (median: 474.75 μg l−1, range: 153.965–2535.80 μg l−1). Studies using animal models also revealed that exposure to high Cu concentrations restrict growth retardation in rat fetuses and the fathead minnow through downregulation of genes associated with growth [41, 42]. And our study found negative effects of Cu on birth weight would increase as the concentration of Cu increased, which also demonstrated elevated exposure levels of Cu in Bangladesh.
The level of Co (median: 0.295 μg l−1, range: 0.011–3.075 μg l−1) found in our study population was similar to or higher than prior studies [11, 43], and we found that Co was inversely associated with birth weight in Bangladesh. Co can accumulate in the body, and long-term exposure, even at a low level, can give rise to adverse health effects in various organs and tissues [44]. In developing countries, Co is present in processing plants, the hard-element industry, and the diamond polishing and ceramic industries, which are widely distributed [45]. Though Mn, Cu, and Co are all essential for human health, our results indicated the presence of excessive levels in Bangladesh that may warrant concern.
Both Y and Er are REEs are emerging contaminants, spreading in the environment widely due to industrialization [46]. REEs can easily cross the placental barrier, thereby affecting fetal growth and development [47]. However, there is little research on this type of pollutant and the potential toxic effects of REE exposure on birth outcome [48]. Our results provide a reference for future research and suggest that more attention should be focused on investigating the toxicity of REEs.
Se, the only essential trace element found to protect against low birth weight, plays an important role in immunocompetence and can protect against oxidative damage [49]. Prior studies demonstrated that Se counters the toxic effects of some elements on birth weight, which was further validated in this study [8, 50]. However, the current study detected a concentration of Se (median) of 15.77 μg l−1 (range: 5.62–47.49 μg l−1), which was much lower than that reported in other studies [51, 52]. For example, a birth cohort study in Japan reported the concentration of Se (median) 191.4 μg l−1 (ranged: 73.9–376.2 μg l−1) in cord blood [53]. This finding warranted consideration, as supplementation of Se for pregnant women in Bangladesh may help to decrease the risk of low birth weight.
Few studies have reported associations between prenatal exposure to metal mixtures and birth weight [54]. In this study, we analyzed the effect of combined element exposure on birth weight and provided evidence that Li is likely a key exposure during pregnancy that contributes to decreased birth weight. Further, BKMR analyses suggested an interaction between Li and the other identified elements; exposure to high levels of Li strengthened toxicity or weakened the protective effect of the other elements on birth weight.
In summary, the present study has the main strengths as follows. First, this study was based on a prospective birth cohort study, which is helpful for exploring causality. Second, we specifically examined the status of 56 elements exposure in cord blood and the associations of individual element with birth weight, identifying seven important elements to the development of fetus. Third, BKMR and WQS analyses were used to explore the effects of elements mixture exposure on birth weight.
Also, there are several limitations in our study. While cord blood is appropriate for the detection of many of the metals analyzed here, the exposure measurements in cord blood may not have captured the most relevant time period of exposure or usual levels of exposure and some metals detection tends to be lower in cord blood [55], which may have contributed to a greater prevalence of non-detects for some of the metals (e.g.: Cd, Lu and Tl). And there may be measurement errors when anthropometric measurements and the measure of elements exposure in cord blood were performed at birth. Also, we cannot rule out the likelihood of contamination in the process of collecting and transport though we have followed a series of standard procedure. It may lead to non-differential exposure misclassification due to the potential measurement errors and contamination. In addition, there are differences in samples and exposure measurements and variation in population characteristics between our study and other studies. Our findings can be a reference about elements exposure during pregnancy, but it must be careful when generalizing these findings to other population. What's more, there still remains largely unknown about the mechanisms of action underlying the effects of element exposure on birth weight, which needs more investigation. Finally, it is necessary to determine whether an exposure threshold exists especially for those essential trace elements based on more inquiries.
Conclusions
In conclusion, we characterized 56 trace element exposure levels in cord serum samples from 745 mother-infant pairs in Bangladesh. Our study demonstrates that exposure to Li, Mn, Co, Cu, Se, Y, and Er are individually associated with birth weight and suggests Li may be a key element that is associated with decreased birth weight. Additionally, we found toxic effects of cumulative exposure to element mixtures (Li, Mn, Cu, Co, Y, and Er) on birth weight. On the other hand, our results suggest that Se supplementation may attenuate the risk of low birth weight by its main protective and antagonistic effects against the toxicity of elements.
Acknowledgments
Z Y, Y W and F C conceptualized the study; X C, L W, and H H designed the study, analyzed the data and wrote the manuscript; R Z, L S, M R, M G M, Q Q, H Y, Y Z, Y W, F C, and D C C collected the samples, processed the samples for analysis, and performed metal level evaluation; R Z, M G M., H Y, and M R contributed to the discussion and revision of the manuscript. All authors approved the final version of the manuscript.
Data availability statement
The data generated and/or analysed during the current study are not publicly available for legal/ethical reasons but are available from the corresponding author on reasonable request.
Ethics approval and consent to participate
The study was described in detail to all participants, and informed consent was obtained before study enrollment. All protocols performed in studies involving human participants were reviewed and approved by the Human Research Committees at Harvard T.H. Chan School of Public Health, Nanjing Medical University, and DCH.
Competing interests
The authors declare that they have no competing interests.
Funding
This study was supported by the State's Key Project of Research and Development Program (2016YFE0204900 to F C), the US National Institute of Environmental Health Sciences (NIEHS) of the National Institutes of Health (NIH) (R01ES015533 to D C C), and a project funded by the Priority Academic Program Development of Jiangsu Higher Education Institutions (PAPD). The sponsors had no role in the design of the study, collection and analysis of data, or preparation of the manuscript.