
Abstract
Many industrial sectors, from pharmaceuticals to consumer products, are required to provide data on their products to demonstrate their efficacy and that they are safe for patients, consumers and the environment. This period of testing typically requires the use of animal models, the validity of which has been called into question due to the high rates of attrition across many industries. There is increasing recognition of the limitations of animal models and demands for safety and efficacy testing paradigms which embrace the latest technological advances and knowledge of human biology. This perspective article highlights the potential for biofabrication approaches (encompassing bioprinting and bioassembly strategies) to meet these needs and provides case studies from three different industry sectors to demonstrate the potential for new markets in the bioprinting community. We also present a series of recommendations to create a thriving bioprinting environment. One that operates at the forefront of science, technology and innovation to deliver improved decision-making tools for the more rapid development of medicines, agrichemicals, chemicals and consumer products, and which may reduce our reliance on animals.
Export citation and abstract BibTeX RIS

Original content from this work may be used under the terms of the Creative Commons Attribution 3.0 licence. Any further distribution of this work must maintain attribution to the author(s) and the title of the work, journal citation and DOI.
Introduction
The development of pharmaceutical and non-pharmaceutical substances across the bioscience sectors (pharmaceuticals, chemicals, consumer product, cosmetic and agribusiness) requires them to be tested to ensure they are safe for patients, consumers and the environment. In some sectors, this period of testing often relies on animal models (primarily rodents). However, animal models are not always accurate predictors of the effects of a new substance in humans or the environment and can be a cause of attrition [1–3]. In drug development, reducing attrition by even a small amount can lead to huge financial savings and increased business growth while importantly ensuring that innovative medicines reach patients who need them [4]. This has called into question the utility and validity of current development approaches across the bioscience sectors, and demands for safety and efficacy testing paradigms to embrace the latest technological advances and knowledge of human biology [5].
Bioprinting or biofabrication (which encompasses both bioprinting and bioassembly strategies) offers a potential technological solution [6]. There is increasing interest from the life science community in the application of this technology to create biomimetic tissues which could be used to replace poorly predictive animal models for better understanding of human health and disease, and in the development of safer and more efficacious chemicals [7–11]. Recent advances in biofabrication has resulted in bioprinting strategies for creating in vitro 3D tissue models (figure 1) that have the potential to accurately recapitulate the complex architecture, cellular heterogeneity and interactions of tissues and organs in the human body [12, 13]. However, as with any new technology, there are always hurdles which need to be overcome before the benefits are realised and it is adopted more broadly. 3D bioprinting and related biofabrication methods is no different, but given the pace at which the field has moved, there have been few opportunities for the community to come together with other disciplines and end users to explore novel areas where bioprinting could have a positive impact. As has recently been highlighted [14], this is an important step in knowledge sharing to understand novel markets for new technologies, and the scientific, commercial, societal and animal welfare benefits that wider application of these technologies brings. Here, we provide a 'call to arms' for the biofabrication community, to facilitate the development and application of bioprinting technologies for improved safety and efficacy testing. Importantly, we have identified and focused on three key organ/tissue areas that require urgent solutions for three industry sectors (i.e.: pharmaceutical, consumer product and agrichemical industries), demonstrating the potential for new markets in the bioprinting community and new opportunities for accelerating innovation to improve models and in turn increase productivity across these industries.

Figure 1 Application of bioprinting technologies to potentially improve drug and chemical development processes (* this does not apply to personal care/cosmetic products). Current drug/chemical development processes rely on a combination of animal and in vitro data to support decision making. The future application of potentially more physiologically relevant bioprinted in vitro models during preclinical development could go a substantial way to realising a future where animal testing is no longer needed in some instances. Summary of the '3D bioprinted in vitro Human Tissues Models' which could be more widely applied in current and future preclinical drug/chemical development processes to reduce reliance on animal models and improve translation to humans. (a) Brain cortical tissue, reprinted from [35], Copyright 2015, with permission from Elsevier, (b) pancreatic islets, reproduced from [36]. © IOP Publishing Ltd. All rights reserved, (c) 3D lung model, reprinted by permission from Macmillan Publishers Ltd: Scientific Reports [37], Copyright 2015, (d) 3D tumour model, reproduced from [38]. © IOP Publishing Ltd. All rights reserved, (e) 3D skin model [27, 39], Reproduced from [27]. © IOP Publishing Ltd. All rights reserved, (f) cartilage tissue [40, 41], reproduced from [40]. © IOP Publishing Ltd. All rights reserved, (g) bone graft, reprinted by permission from Macmillan Publishers Ltd: Nature Biotechnology [42], Copyright 2016, (h) cardiac tissue [43, 44], reproduced from [43]. © IOP Publishing Ltd. All rights reserved, (i) microvascularature and vascularised thick tissue [45] Copyright (2016) National Academy of Sciences, (j) liver tissue, reproduced from [8]. © IOP Publishing Ltd. CC BY 3.0, (k) kidney renal tissue, reproduced from [46]. CC BY 4.0., (l) 3D vasculature, from [47]. © The authors, some rights reserved; exclusive licensee American Association for the Advancement of Science. Distributed under a Creative Commons Attribution NonCommercial License 4.0 (CC BY-NC) http://creativecommons.org/licenses/by-nc/4.0/.
Download figure:
Standard image High-resolution image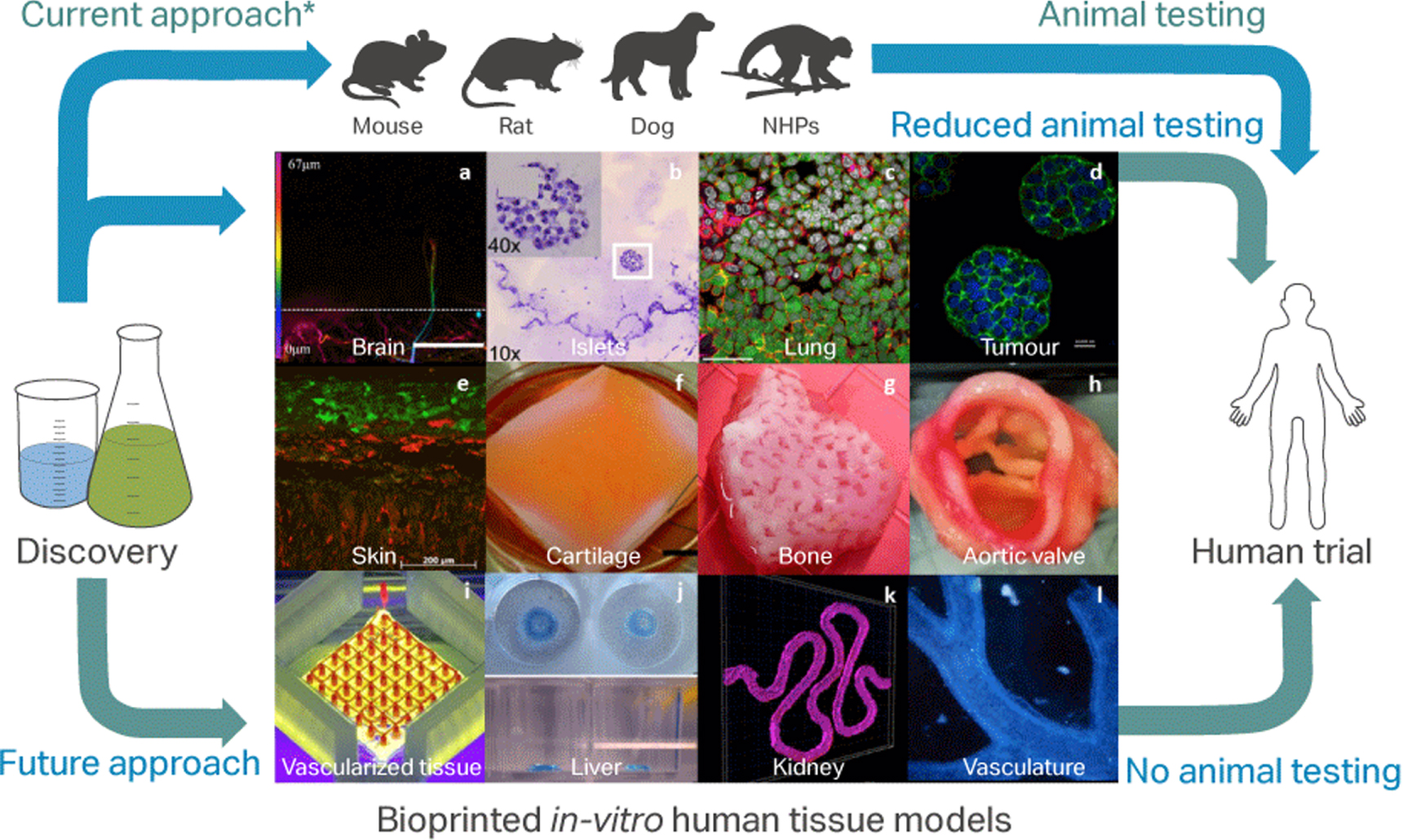{kind=link}
We also provide a series of recommendations to create a thriving global bioprinting environment. One that operates at the forefront of science, technology and innovation to deliver improved decision-making tools for the more rapid development of medicines, agrichemicals, chemicals and consumer products, and which may reduce our reliance on animals.
Case study 1—in vitro models of liver structure and function for assessment of hepatotoxicity and carcinogenicity in plant protection product development
The continuing growth in global population, together with rising calorie consumption, has resulted in a potentially unsustainable demand for food. It is the vision of agribusinesses to bring greater food security in an environmentally sustainable way to help meet this demand for yield gain. As such, their product portfolios include a broad range of plant protection products (PPPs; e.g., herbicide, insecticide, or fungicide) which require comprehensive mammalian toxicity evaluation, including carcinogenicity studies, before they can be registered in most regions of the world.
It is a requirement that all active substances be tested in at least two species (usually rat and mouse) for their potential to act as carcinogens. The liver is a common target organ in agrochemical carcinogenicity studies. Hepatocellular hyperplasia is a common injury response to chemical exposures in rodent toxicity studies and may result in unfavourable toxicity profiles in long term toxicity studies. Current approaches for examination of liver toxicity require samples taken from repeat dose in vivo studies, but in a conventional testing paradigm such studies are conducted only after other in vivo toxicity studies have been completed. Earlier identification of unfavourable areas of chemistry may reduce the number of animal studies conducted with compounds which are ultimately determined to be unsafe or unregisterable.
However, the utility of these studies has been called into question. Carcinogenicity studies run in rats are not necessarily predictive of the result of similar studies run in mice [15], and liver tumours in rodent models are not conclusive evidence that a compound will exert a carcinogenic effect in humans (as a result of rodent-specific tumorigenic mechanisms). To examine the human relevance of tumours observed in rodent carcinogenicity studies, in vitro and in vivo models are used to establish the adverse outcome pathway (AOP) underlying the observed effects [16]. Once established in rodents, the sequence of causative key events in the AOP can be interrogated across species to examine the relevance of rodent toxicities to humans. Currently the establishment and cross species interrogation of key events in AOPs is a complex, iterative undertaking requiring a number of animal studies.
Whilst current in vitro models are able to provide insights into the AOPs of liver toxicity, existing models do not accurately reproduce the architecture of liver tissue and often do not include the full range of cell types present in vivo (including hepatocytes, cholangiocytes, Kupffer cells, liver endothelial cells, and hepatic stellate cells). As a result, existing in vitro liver models are generally not suitable for histopathological analysis, limiting the potential for validation of these models against existing in vivo toxicity databases and their ability to predict the outcome of in vivo studies. Furthermore, the absence of architecture and use of limited cell types in existing models prevents accurate mimicry of tissue microenvironments, potentially reducing model predictivity.
Bioprinted organ models and tissues could potentially be used to both establish AOPs and as a tool to facilitate evaluation of the relevance of rodent tumours to humans, increasing the confidence in safety assessments and reducing the reliance on animal models. This could help guide early stage agrochemical research projects away from toxic areas of chemistry through early detection of hepatic toxicants and structure-activity relationship building. Rapid advances are being made in this area [17–19], but there still remain a number of critical considerations which need to be accounted for during future model development to maximise the potential of these tools in the context of safety assessment of PPPs—see table 1.
Table 1. Comparison of existing in vivo and in vitro technologies for studying liver injury.
| Property | Achievable in vivo | Achievable in vitro |
|---|---|---|
| Mimicry of normal human liver metabolic function | Yes, although species differences in metabolism can occur | Yes, but results are sometimes of unclear relevance to in vivo |
| Assessment of molecular endpoints (protein induction, mRNA) | Yes | Yes, but results are sometimes of unclear relevance to in vivo |
| Detection of cell proliferation | Yes | Yes |
| Suitable for histopathological examination | Yes | No |
| Assessment of organ weight changes | Yes | No |
| High temporal resolution measurements (<1 day) | Possible but not common outside metabolism studies | Yes |
| Replicate number | Limited by welfare concerns | Limited by practical concerns |
To be useful models for mode of action (MOA) investigation and as a predictive tool for compound development, the response of bioprinted constructs to hepatotoxins should be demonstrated to mirror the physiological, histological and biochemical responses observed in humans and rodents. The properties that a bioprinted liver model should exhibit in order to function as a predictive model are likely to require further investigation, however factors including metabolic capability (e.g. expression and activity of phase I and II enzymes), gene and protein expression (particularly of key nuclear receptors including the peroxisome proliferator activation receptors, constitutive androstane receptor, pregnane X receptor, retinoid X receptor, aryl hydrocarbon receptor, farnesoid X receptor, and glucocorticoid receptor) and cellular structure (open questions include the necessity of Kupffer cells in modulating responses to hepatotoxicants) are likely to prove important in model development.
Details regarding the manufacture of bioprinted constructs, such as whether constructs are created in the presence or absence of a scaffold are unlikely to be a serious concern for industry, as the primary concern for these models will be around predictivity and validation rather than method of manufacture. How amenable the tissue is to histology is also an important consideration in being able to back translate responses to existing liver toxicity data and provide a degree of confidence in the ability of the model to predict human responses. Whilst precursor events are commonly observed in sub-acute and sub-chronic toxicity studies, most liver carcinogenicity observed with agrochemicals is the result of chronic exposure. As such the longer term stability of the model (up to 28 days) in culture is important to provide sufficient time course data to be able to predict chronic effects and support the development of appropriate AOPs.
Case study 2—human-relevant models of respiratory disease in pharmaceutical drug development
The pharmaceutical industry is facing considerable challenges in the development of new safe and efficacious innovative medicines. Productivity has declined steadily over the last two decades, despite the investment in drug development doubling every nine years over the last 60 years. Only 10% of drug candidates entering the clinic achieve US Food and Drug Administration approval [20] and, according to some studies, it now costs approximately $2.6 billion to develop a drug [21]. A number of factors contribute to the high attrition rate and costs in drug development, including higher regulatory hurdles for safety and efficacy and commercial considerations including reimbursement strategies as well as strategic portfolio decisions driving project termination. But a substantial proportion of this failure can be attributed to the lack of safety or efficacy, suggesting the preclinical models used to assess these poorly translate to the clinic [22].
Respiratory disease remains an area of considerable unmet medical need with significant barriers to new drug development [23]. Many of the new respiratory drugs that have failed in the clinic have performed well in preclinical animal models, suggesting more predictive models and tools based on the latest technologies, including bioprinting, are required. But what these models should look like will clearly depend on the question being asked, and what particular respiratory disease you are studying. A 'one size fits all' model will not work, and therefore engagement and collaboration between the bioprinting community and end-users early in model development is essential for delivering bespoke models with utility.
Diseases such as asthma and chronic obstructive pulmonary disease are complex, heterogeneous diseases with diverse aetiologies. Not one single model is likely to replicate all of the necessary features to recreate these diseases in vitro, but there are some common features that are essential starting points. These include being able to model airway hypersensitivity and inflammatory cell recruitment. For example, bioprinting the bronchiolar epithelium should include not only the simple ciliated columnar cells but also secretory Clara cells, as well as neuroendocrine cells. Alveolar units should comprise Type I cells and Type II cells while pulmonary vascular tissues should include endothelial cells from different vascular structures, smooth muscle cells, and adventitial fibroblasts [24]. Importantly, any bioprinted lung mimetic should incorporate cells from the innate immune system or even adaptive immune systems if studying a particular pathogen to aid our understanding of the immune processes which drive respiratory disease. Given the chronicity of respiratory disease, it is important that bioprinted material can be used over a prolonged period of time and therefore demonstrate viability of weeks and preferably months, rather than days. As our ability to stratify patient phenotypes improves, we also require models that represent the heterogeneity of patient subpopulations. Such an approach is also likely to require mathematical modelling to determine the appropriate number of variants to create and study.
Understanding the basic anatomical and cellular components for bioprinting lung models suitable for drug discovery is the first step towards creating useful models for improved efficacy and safety testing without animals. Working collaboratively with the end-users will ensure that material is printed and models are built that address the gaps evident with current models. Related to this, by working in a partnership the bioengineering community will understand how and why the models are used and at what point in the drug discovery/development pipeline they will be deployed. Of particular value is the bioprinting of cells for use within phenotypic screens that elucidate new targets or drive a greater understanding of biological targets early in preclinical drug development. This has the benefit of enabling companies to identify early those compounds destined to fail and remove them from development before the more expensive animal testing stages—fail early; fail cheap is the commonly used mantra. For these early screens where thousands of potential therapeutics will be assessed to identify if they can alter the phenotype of a cell or tissue in a desired manner, the models need to be fairly simple to meet the demands for high-throughput and high-content systems and importantly cost-effective and highly reproducible. However, if bioprinted material is employed in the latter stages of discovery, for example prior to candidate drug nomination, a lower throughput, more complex system is preferred. In this scenario, the model should try to emulate physiological or pathophysiological responses that are not detectable in animal models or other complex in vitro model systems.
Case study 3—better models to assess the benefits and safety risks of consumer products on skin
The consumer goods industry spans a number of different product types, including foods, drinks, homecare and personal care products. Since 2013, legislation in the European Union has banned the marketing of cosmetics and personal care products that contain ingredients that have been tested on animals. For some toxicity endpoints (e.g. skin corrosion, eye irritation and androgen receptor activity), Organisation of Economic Cooperation and Development test guidelines exist to allow data generation without using animals. However, for other important toxicity endpoints, no guidelines currently exist. The marketing ban has the potential to stifle innovation in the sector and so there has been a concerted effort towards the development and application of new in vitro approaches by the personal care products industry. Bringing greater focus on human relevant, in vitro MOA safety (and efficacy) assessment and embracing Safety Science in the 21st Century framework approaches [25, 26].
The majority of homecare and personal care products interact with the skin either intentionally or as a consequence of use in other capacities, and so assessing the possible effects of these chemicals at both the skin surface and underlying structures is an essential part of consumer product development. In vitro cell culture of human cells plays an important role in both the identification of new targets and leads and in assuring their safety. Numerous 2D and 3D model systems exist for this purpose, but their utility can sometimes be limited because of their (i) cellular composition (primarily keratinocytes and fibroblasts), (ii) lack of appendages and other macrostructures (e.g. hair follicles, sebaceous glands, vascularisation) and (iii) inability to represent other cell types in the skin (e.g. immune cells, adipocytes, dendritic cells, melanocytes etc). In this context, current 3D systems have only limited value in enabling the identification of new targets (e.g. in a hair biology/skin ageing context where the presence of macrostructures and vascularisation are key determinants of in vitro to in vivo functional equivalence); neither do they represent sufficient human biology to advance our mechanistic understanding of adverse events (e.g. skin sensitisation, where immune function is often poorly represented in the available model systems).
Bioprinting offers the ability to automatically fabricate robust and reproducible 3D skin models with improved human relevant functionality and which possess critical attributes of the target tissues they represent [27, 28]. These tissues can be configured to mimic the cell density of the target tissue and to be composed solely of the appropriate cells and extracellular matrix they produce. Spatially defined deposition of cell types also enables the design and fabrication of tissues that recapitulate key architectural features of the target tissue in vivo. This spatial patterning and cell alignment is crucial to the normal functioning of most tissues, enabling cell–cell communication to be more effectively emulated. More highly complex skin models containing blood vessels and nerve fibres are potentially feasible, allowing for questions of safety and efficacy to be answered in a more in vivo-like context—see box 1.
It is unlikely that it will be possible to develop a single model that is capable of representing the entirety of human relevant biology, and that bespoke assays may be required to address, for example, effects at the level of the hair follicle [29], or effects exploring aging biomarkers, or immune responses in the skin. It is clear that certain solutions/models are further off than others in terms of their development and application. Recapitulating functional structures in the skin (e.g. sebaceous glands and hair follicles) is on a longer term horizon than say the introduction of immune competent cells into models, although this too is no trivial endeavour. Maintenance of immune cells in skin models is a key challenge as they are often short-lived and are 'recruited' to the site of function.
Being able to measure the exposure of chemicals via the dermal route is very important in any skin model. Current approaches rely on the use of ex vivo skin samples which lack functional vasculature, and so penetration is measured as a function of transit through the skin. Building in more human relevant functionality, future bioprinted skin models should incorporate tissue printing around pseudo-blood vessels to support more relevant in vivo-like exposure studies. The availability and access to ex vivo skin is often limited, therefore future bioprinting of 3D skin samples could potentially address this need and bring greater consistency/standardisation concerning the tissue supplied. Other safety endpoints of importance that should be considered in the development of bioprinted skin models include standard measures of cytotoxicity, genotoxicity and allergy. Immunotoxicology is of particular interest because of the deficiencies acknowledged in currently available 3D models regarding the absence of immune function and critical cell types (for example dendritic cells, mast cells, T-cells). 3D bioprinted models able to incorporate and retain these cell types within the tissue construct would represent a significant step forward in consumer product development.
Conclusions and recommendations
There are clear opportunities for the application of bioprinting approaches to support pharmaceutical and non-pharmaceutical chemical development, and there is good appetite from both the bioprinting and life science communities to realise this [14]. Bioprinting potentially offers key advantages in the development of more functionally relevant/predictive models for basic and applied research, when compared to more traditional 3D cell culture approaches which do not go beyond simple prototissue models (see table 2 and [12, 13]). Although the case studies presented here originated from different industry sectors, the development of well-characterised, reproducible, affordable, human relevant bioprinted models of any organ/tissue would be welcomed across the life science sectors.
Table 2. The opportunities for, and hurdles to, wider adoption of bioprinted models for efficacy and safety testing in drug and chemical developmenta.
| Opportunities | Hurdles |
|---|---|
| The potential for improved reproducibility of tissue fabrication—especially important when being used to assess safety/efficacy of compounds reliably over time | There is a current lack of validation of existing models to support wider uptake and acceptance by decision makers and regulatory authorities |
| The ability to print using human material [8] and incorporate greater structural complexity, e.g. incorporating sweat glands, hair follicles and other appendages in skin models, and close proximity bioprinting of immune and structural cells in lung models | Current bioprinting equipment is mostly bespoke, encouraging a wide diversity in devices and limiting their use in a wide range of applicability domains |
| The potentially improved functionality due to incorporating greater structural complexity | The perceived reluctance of regulatory authorities to accept data derived in non-animal models to support clinical trial applications |
| The potentially more predictive responses generated in more in vivo-like, human tissue models | A lack of opportunities for cross-sector and –discipline communication to understand user needs and bioprinting capabilities |
| The speed, relative ease and reduced cost at which tissue can be fabricated | A lack of standardisation of models and the criteria for assessing model performance |
| The potential for personalised bioprinting as a route to enable and accelerate the realisation of personalised medicine | Inertia and a reluctance to embrace change and move away from currently used in vitro and in vivo models |
aThese represent the consensus views of the biofabrication and industry community as discussed at [14].
Box 1. Five key areas where bioprinted skin models will be especially beneficial.
| Improved speed and accuracy for identification of lead actives. Improved consistency and biological relevance of these models and the capacity for high throughput production may deliver superior screening technology, leading to more effective identification and validation of lead molecules. |
| More predictive tissue models for investigative research and target identification. Building multi-cellular models, more closely predictive of the in vivo tissue, will allow tissue physiology and function to be investigated more effectively, leading to better identification of lead targets. |
| More biologically relevant models for assessing effects on pathways. Assessing the safety of new lead molecules using a pathways-based approach will benefit from an increased availability of human-relevant biological models to use, particularly in pathways/organs that are poorly covered by currently available models. |
| Potential replacement for limited human tissue supply. The incorporation of iPS cells into these models will provide an alternative source of cells for incorporation into the 3D models. An inexhaustible supply of identical cells will be available for repeat systems modelling and higher throughput testing. |
| Better prediction of clinical outcomes. The increased relevance of these models to the in vivo tissue has the potential to decrease lead time and deliver a higher proportion of successful clinical outcomes. |
However, the critical components of in vivo biology described in the case studies are not likely to be well known by the engineers developing the bioprinting technology capable of creating these models. Therefore, a more concerted effort is needed to support these communities in coming together at the start of model development to save time and resources while maximising the expertise available in understanding end-user requirements and technological capabilities. Many hurdles exist to this (see table 2), and some of these may be more easily overcome than others, but the potential benefits to the science base, chemical development and the 3Rs are many.
Recommendations to address these hurdles and maximise the opportunities are described below. These focus on better cross-sector and -discipline engagement in (i) defining the problems that can be solved together; and (ii) developing strategies to support acceptance of bioprinted models by senior decision makers. A key thread linking these themes is the need to form longer-term partnerships between large companies (e.g. pharmaceutical, consumer products, etc), SMEs, and universities; and it is important that funders and regulators also play their part in supporting this.
- 1.Define a clear problem statement The life science community needs to be more coordinated to work in partnership to define focussed, translatable and tractable problems that can be solved using bioprinted models. Central to this is the need to provide a forum for potential industry end-users to work collaboratively in a pre-competitive manner to define and prioritise which disease-specific bioprinted models they would like to have access to and the minimum starting criteria (structure and function) for those models to be useful. Demonstrating successful examples of the application of viable bioprinted models to highlight scientific and commercial feasibility and industrial 'pull-through' will help to encourage the wider engagement of both the academic and industrial sectors. Expanding collaborative programmes for challenge-led innovation and strategic funding (e.g. CRACK IT [30]) will also help to engage and support technology developers and multidisciplinary teams in developing bioprinting approaches for solving biology challenges.
- 2.Supporting validation and senior decision maker acceptance through collaboration Validating new models is an important and ongoing phase of model development, during which physiological baseline data and responses to compounds are assessed and compared with clinical outcomes. Establishing an approach for technology developers and end-users (cross-company and -sector) to work collaboratively on defining a compound library (including associated in vivo data and mechanistic/pharmacology information where possible) for testing bioprinted models for efficacy and safety testing is essential in supporting this validation process. Expediting the often lengthy validation process requires a tiered approach that would firstly demonstrate industry's willingness to use, and acceptance of, bioprinted models in safety and efficacy decision making. Regulatory acceptability of a bioprinted model for decision making is crucial to enable successful registration of products and as confidence grows in this sector, acceptance by the regulatory agencies would likely follow. Establishing an approach to support demonstrators within institutions or companies to generate interest and provide access for trial use to familiarise potential users would engender greater confidence in the utility of bioprinted models and encourage potential uptake. Regulatory acceptance is an important factor when considering whether or not to adopt a novel technology for decision making. Therefore it is important to support wider use of existing mechanisms for technology developers and end-users to engage with regulators on model development and to receive feedback on the potential for safety data generated in bioprinted models to be accepted by regulatory agencies. Both the UK Medicines and Healthcare products Regulatory Agency (MHRA; [31]) and European Medicines Agency (EMA; [32]) have safe harbour approaches to facilitate this. However, as a global industry, without engaging additional regulatory agencies in embracing similar approaches for greater dialogue with technology developers and end-users on model development and application it may be difficult to convince some companies and sectors to adopt novel bioprinting models.
- 3.Supporting cross-sector and -discipline collaboration There should be greater opportunities to enable closer working relationships between scientists with the diverse skill sets necessary for the successful development and application of bioprinted models, for example, engineers, biologists, chemists, materials scientists and industry end-users. Specific forums to facilitate this will enable better understanding of end-user model requirements and bioprinting capabilities and reduce the potentially unrealistic expectations of what the technology can deliver. Funding will always be a key driver for this collaborative approach to research and development, so continued and increased collaboration between funders for example in the UK the NC3Rs, Innovate UK, and the Research Councils to nurture long-term partnerships between leading scientists, centres of excellence, and industry, should be encouraged. As should more multi-agency research funding calls recognising the multidisciplinary nature of bioprinting development and application.
- 4.Adding value to in vitro modelsApplying bioprinting approaches in the creation of more human-like cell culture models, for example by incorporating immune cells to investigate modulation of the immune response; and hair follicles in skin models, relies on provision of opportunities for focused cross-sector and -discipline collaboration. Going beyond this, it is necessary to also support interdisciplinary collaboration to maximise the utility of other technologies through the incorporation of more human relevant bioprinted models. For example, microfluidic organ-on-chip platforms have become an important tool to understand the role of cellular interactions and the impact of potential therapeutics to model and treat disease [33]. Because of its versatility, 3D bioprinting has emerged as a leading tool for fabricating in vitro biomimetic devices that capture some of the more complex functions of the human body [34]. Conversely, incorporating other approaches such as mathematical and in silico modelling within bioprinting strategies can help inform and speed up this biomimetic model development. Finally, to achieve a step-change in scale-up and manufacture of bioprinting-based technologies and models, there must be increased focused activity to nurture long-term, cross-discipline (industry/SME/academia) collaboration.