

Abstract
Extreme heat has tremendous adverse effects on human health. Heat stress is expected to further increase due to urbanization, an aging population, and global warming. Previous research has identified correlations between extreme heat and mortality. However, the underlying physical, behavioral, environmental, and social risk factors remain largely unknown and comprehensive quantitative investigation on an individual level is lacking. We conducted a new cross-sectional household questionnaire survey to analyze individual heat impairment (self-assessed and reported symptoms) and a large set of potential risk factors in the city of Berlin, Germany. This unique dataset (n = 474) allows for the investigation of new relationships, especially between health/fitness and urban heat stress. Our analysis found previously undocumented associations, leading us to generate new hypotheses for future research: various health/fitness variables returned the strongest associations with individual heat stress. Our primary hypothesis is that age, the most commonly used risk factor, is outperformed by health/fitness as a dominant risk factor. Related variables seem to more accurately represent humans' cardiovascular capacity to handle elevated temperature. Among them, active travel was associated with reduced heat stress. We observed statistical associations for heat exposure regarding the individual living space but not for the neighborhood environment. Heat stress research should further investigate individual risk factors of heat stress using quantitative methodologies. It should focus more on health and fitness and systematically explore their role in adaptation strategies. The potential of health and fitness to reduce urban heat stress risk means that encouraging active travel could be an effective adaptation strategy. Through reduced CO2 emissions from urban transport, societies could reap double rewards by addressing two root causes of urban heat stress: population health and global warming.
Export citation and abstract BibTeX RIS

Original content from this work may be used under the terms of the Creative Commons Attribution 3.0 licence.
Any further distribution of this work must maintain attribution to the author(s) and the title of the work, journal citation and DOI.
1. Introduction
Heat stress has been recognized as one of the major direct and adverse impacts of climate change on urban populations worldwide (IPCC 2014). Large urban agglomerations are particularly affected due to the urban heat island effect. Negative effects of extreme heat on human health range from decreased well-being and morbidity to heat-related mortality. Heat stress risk is currently increasing and expected to further increase due to three assumed root causes—urbanization, global warming and population aging. Urbanization leads to higher proportions of people exposed to, and an intensification of, the heat island effect. Global warming is expected to bring stronger and more frequent heat waves. Population aging is expected to increase the proportion of sensitive people (Wilhelmi and Hayden 2010, Huang et al 2013, Leichenko and Solecki 2013, Fernandez and Creutzig 2015).
Empirical evidence for negative health impacts has been gained mainly through the statistical analysis of temperature and mortality (or hospital admission) data. Previous research identified strong statistical correlations between heat and mortality for many cities worldwide (Oudin Åström et al 2011). Underlying causes and susceptibility, however, remain largely unclear since heat is generally not documented as cause of death or disease (Hajat and Kosatky 2010, Kenny et al 2010), and it is impossible to study mortality under laboratory conditions (Robine et al 2012). Several studies used large mortality data sets and related them to the personal characteristics provided in death certificates (Stafoggia et al 2006, Medina-Ramón et al 2006, Chan et al 2012). Death certificates may detail pre-existing medical conditions. However, for an examination of individual risks, they do not provide sufficient information on personal backgrounds (other than general characteristics like age, sex, level of education etc). Few mortality studies attempted to reveal individual risk factors via intra-urban spatial differentiation of the population and its living environment (Harlan et al 2006, Klein Rosenthal et al 2014). However, they were also restricted by data availability issues (Reid et al 2009, Yardley et al 2011, Harlan et al 2013). Thus far, the clearly dominant and commonly identified risk factor was age, and elderly people were commonly identified as being the most sensitive group (Reid et al 2009, Romero-Lankao et al 2012). Some studies reported chronic disease as a main risk factor; very few reported environmental or socio-economic risk factors (Romero-Lankao et al 2012). On the other side of the scale laboratory-based studies provide evidence for the physiological relationship between heat and physical impairment (Kenney and Munce 2003, Kenny et al 2010). Few studies reported qualitative interviews of individuals and a single quantitative survey (Wolf et al 2010, Bittner and Stößel 2012, Großmann et al 2012).
There is a significant research gap with regard to the vulnerability of the population, and more holistic assessments of impacts on health and well-being (Thomas et al 2014). Research still lacks more comprehensive and integrated quantitative investigations of physical, behavioral, environmental, and social risk factors (Oudin Åström et al 2011, Yardley et al 2011, Romero-Lankao et al 2012). To identify major risk factors and to infer risk groups, research needs to overcome data limitations at aggregated spatial and individual scales through quantitative surveys of individuals (Reid et al 2009, Wilhelmi and Hayden 2010, Wolf et al 2010).
Self-rated health assessments in questionnaire surveys are powerful health status indicators (Mossey and Shapiro 1982, Miilunpalo et al 1997), recognized as such by the World Health Organization and in a wide range of scientific literature (Wannamethee and Shaper 1991, Jylhä 2009, Cohen et al 2015, Maheswaran et al 2015). Even though observational studies are imperfect due to unquantifiable biases, quantitative surveys of self-assessed effects of heat still appear as powerful tools to overcome the knowledge gap in urban heat stress research.
The aim of this study was to create a new dataset to find associations of heat stress with related risk factors on the individual level. To this end, we set up a quantitative field survey to analyze self-assessed heat stress and a comprehensive set of potential risk factors. We developed a large set of potential risk factors as identified through literature research and continuous exchange with experts from different scientific fields. The objective was then to explore the rich and multi-faceted dataset and to identify the major heat stress risk factors across the vulnerability dimensions: physical sensitivity, environmental exposure, and adaptive capacity.
2. Methods
2.1. Study site
The administrative area of Berlin, the capital of Germany, is inhabited by 3.45 million people over an area of 892 km². It is the largest city in Germany and represents one of the major metropolitan areas in Europe, with a clear urban heat island effect (Dugord et al 2014). Berlin is located in the temperate climate zone (52°28'N, 13°18'E), affected by both maritime and continental climatic characteristics. The annual average temperature is 9.5 °C and the annual rain fall is 590 mm. The proportions of green spaces and open water, as well as building type and building density, vary largely within the city boundaries. Inner-city areas are compact and densely populated. In Berlin, these areas are dominated by late-19th century housing block developments. Residents have varying levels of social status, similar to most European cities (Honold et al 2012). In 2006 and 2010, Berlin was struck by severe heat waves, which were accompanied by strong increases in death counts (Schuster et al 2014).
2.2. Heat stress survey
Survey design
We developed a cross-sectional, quantitative heat stress survey to investigate individual-level heat impairment and potential risk factors. For questions regarding the survey please contact the main author.
We conceptualized our analysis along the general risk concept common in the climate change community, where heat stress risk is defined as a function of hazard and vulnerability (Romero-Lankao et al 2012, Scherer et al 2013). We developed a model for the concept based on variables that interact with one another along a functional chain of urban heat stress (figure 1). While hazard is determined by the heat impact (the local climate) an urban area is exposed to, vulnerability is determined by the exposure, the sensitivity, and the adaptive capacity of the urban population. Exposure describes how individuals or population samples are exposed to the heat island in terms of its intra-urban differentiation as induced by variations in land use (Dugord et al 2014) or individual living space exposure. Sensitivity refers to individuals' physiological constitution and describes how sensitive people are when exposed to the heat impact. Individual adaptive capacity describes the degree to which people are capable of implementing adaptive measures to counterbalance exposure or sensitivity driven heat impacts based on awareness and resources.
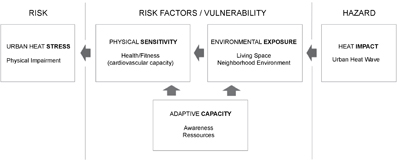
Figure 1 Functional chain of urban heat stress and underlying concept for this study. Risk concept, vulnerability dimensions and major indicator groups per dimension.
Download figure:
Standard image High-resolution imageTo assess urban heat stress, the survey included a series of questions on participants' appraisal and self-assessed consequences of summer heat, referring to the heat waves in 2013. We investigated self-assessed heat impairment as a dependent variable by querying the participants for their perceived level of heat impairment during hot summer days, since self-assessed health is regarded as the most informative health measure in population studies (Jylhä 2009, Maheswaran et al 2015). It was assessed on a five-point Likert scale from 1 = not impaired at all to 5 = very strongly impaired, following standard survey procedures like the SF-36 health survey to assess general physical health (Cohen et al 2015). We further assessed personal emotions towards summer heat and the quantity of related health symptoms as control variables.
We aimed at arranging a questionnaire that allows for comprehensive exploration of potential risk factors. The extensive set of risk factors covered all three vulnerability dimensions (tables S9–S12). Risk factors were not designed for further causal inference but rather for locating empirical individual-level dynamics on heat stress risk factors for future studies. The variables were selected based on the heat and health literature at different spatial scales and thematic detail. We designed additional questions about potential risk factors that we assumed to be influential as well, as arose from continuous exchange with experts from different scientific fields (see the acknowledgements).
Sampling design, implementation, response rate
We were unable to use a probabilistic/randomized survey design for several practical and ethical issues. Instead, we used a cluster-sampling design to acquire a sample that would be as non-arbitrary and structured as possible, adapting the approach of Honold et al (2012) (see supplementary material, part 2). We conducted the survey from 10–18 August 2013, right after the longest heat wave of the summer of 2013 in Berlin, which took place from 2–7 August, as documented by the heat warning system of the German Meteorological Service. At that time, participants had recently experienced urban heat stress and its impairments. They were required to answer until 13 September 2013, thus providing about four weeks as sufficient time in case of temporary absence. The survey was conducted in accordance with human research ethics according to the declaration of Helsinki (WMO 1964). We received a high sample size (n = 474) from 17 August to 13 September corresponding to a response rate of 17.7% valid questionnaires. For further details see supplementary material, part 2.
Sample characteristics and data preparation
We used predominantly standardized scales for data collection. Participants were 46 years old on average, 61% were female, and the net income per household was 2235 €. For a complete overview of the variables examined and the characteristics of the sample, see supplementary material, part 2. Data preparation involved the calculation of specific additional variables that we did not inquire directly, e.g. body mass index (BMI) (see supplementary material, 2.3). A comparison of the selected risk factors between the sample and the full Berlin population is provided in supplementary material, part 3.
2.3. Data analysis
For our exploratory data analysis, we studied the dependent variable self-assessed heat impairment using a five-point Likert scale. We checked for its general agreement with other potential dependent variables such as personal emotions towards summer heat, the individual awareness of heat risks, and the total quantity of reported symptoms by calculating the correlation. We used a three-step approach for the exploration of risk factors.
1). Variable reduction
We trimmed our large list of independent variables by using a data-driven approach. We cross-correlated all independent variables within the three risk dimensions to explore variable interdependences. Further we calculated bivariate correlations with the dependent variable heat impairment to eliminate the variables that did not show significant bivariate correlations. Thus we focused on the observation of variables that could represent independent risk factors.
2). Bivariate correlation assessment
We used the bivariate correlation analysis to assess the strength of the association with heat impairment for each explanatory variable. We used Spearman rank correlation to assess effect magnitude (expressed as rho) and significance for both the continuous and ordinal scaled variables to achieve comparability. We used the Fisher Yates Exact test to test the dichotomous variables for significance (Field et al 2012). We explored each variable more closely using box-plots, mosaic plots, and error bar plots. We assessed correlations among the strongest risk factors within each risk dimension to identify potential confounding effects on heat impairment.
3). Regression modeling
We calculated regression models to reduce problems of multiple-testing linked with bivariate data analysis. We used ordered logistic regression (OLR) because it suits the ordinal nature of our dependent variable (even though in social science research this data scale is often accepted as quasi-metric). OLR has limitations regarding the model output, e.g. no coefficient of determination. Due to the expected multi-collinearity among the variables we expect moderate explanatory power. We converted the coefficients into odds ratios to enhance the interpretation of the outputs following a documented procedure (UCLA 2017). We calculated OLR models for different sets of independent variables. In an effort to further reduce multi-collinearity we iteratively reduced the variables to the ones that were a) least correlated with one another and b) returned the strongest odds ratios.
Finally, we compared the means and the frequency distribution of our sample with available Berlin-wide data to check the qualitative agreement of the characteristics of our sample with the Berlin population. All calculations were completed using R software, version 2.15.2.
3. Results
In this section we focus on the most relevant results of our exploratory study. A complete overview of all explored variable associations is accessible in the supplementary material.
3.1. Self-assessed heat impairment, symptoms, and general heat appraisal
The dependent variable self-assessed heat impairment correlated both in magnitude and significance with the control variables emotions towards summer heat (rho 0.73, p-value < 2.2 × 10−16) and the quantity of health symptoms (rho 0.46, p-value < 2.2 × 10−16) as a quantitative variable.
3.2. Risk factors of urban heat stress
Physical sensitivity variables returned the strongest correlations with heat impairment (table S1, available at stacks.iop.org/ERL/12/044021/mmedia). We observed particular strong associations for health and fitness variables. Among others these included self-assessed health and self-assessed fitness, body mass index (figure 2), pre-existing diseases (online supplementary figure S1), and amount of cycling or active travel. The association with age, however, was weaker. There was no association with gender. Ordered linear regression (OLR), variable cross correlation, and odds ratio calculation indicated that self-assessed fitness was the most predictive of all variables in the health domain (online supplementary table S4, S5).

Figure 2 Level of heat impairment by body mass index (BMI). Box-plots indicate an association between heat impairment (Likert scale: 1 = very low, 5 = very high) and BMI that is monotonic and stronger than for age and heat impairment.
Download figure:
Standard image High-resolution imageEnvironmental exposure variables only returned significant associations when linked to the personal living space, not to the neighborhood environment (online supplementary table S2). We found the strongest association for the geographic orientation of bedroom windows (figure 3) and further ones for apartment story and building types. The results of the OLR further supported these observations (table S4, S5).
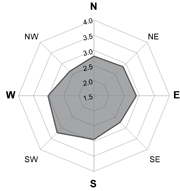
Figure 3 Level of heat impairment by geographic orientation of bedroom windows. The spider plot shows highest impairment levels (Likert scale: 1 = very low, 5 = very high) for south-western orientations.
Download figure:
Standard image High-resolution imageAdaptive capacity variables returned relatively strong associations for risk awareness and adaptation measures. Interestingly, these were positive (online supplementary table S3). We found significant negative correlations and relevant odds ratios (table S5) for some resource-related variables. Classic socio-economic variables were insignificant.
3.3. Variable associations for age and health/fitness
We particularly investigated variable cross-correlations for age and health/fitness.
All variables related to health and fitness were strongly correlated with each other, as described in the supplementary material, 1.3.
Age had relatively strong negative associations with health/fitness variables (online supplementary table S6). For male participants, we observed an interesting bi-directional trend of impairment and age (figure 4). While younger persons reported medium levels of heat impairment, there was a tendency for older ones to report levels on the two ends of the scale, either impaired or non-impaired (figure 4(a) and (b). For males aged 65 and older (figure 4(c)), the highest level of heat impairment was not associated with the oldest respondents. Age also returned significant correlations with most relevant exposure and adaptive capacity variables. However, bedroom orientation (exposure) and household size (adaptive capacity) were not correlated with age (online supplementary table S7).

{kind=link}
{kind=link}
{kind=link}
Figure 4 Level of heat impairment by age for males. Box-plots indicating the level of heat impairment (1 = very low, 5 = very high) for male participants: (a) complete sample, (b) under 65 years, and (c) over 65 years. The graphs show non-monotonic relationships for heat impairment and age for males.
Download figure:
Standard image High-resolution image{kind=link}
4. Discussion
Our study aimed at identifying individual risk factors for urban heat stress using a unique individual survey. Based on a quantitative survey of self-assessed heat impairment, we assessed and explored a large set of potential risk factors. Our survey revealed several previously undocumented risk factor associations. Our major result is that individual physical sensitivity, mainly determined by health status and physical fitness, rather than age per se, was the dominant health risk dimension. This observation may yield a focus shift in future heat stress adaptation research and policy.
4.1. Self-assessed heat impairment as heat stress indicator
Our study uses self-assessed heat stress to measure the vulnerability of the population on the individual level. It represents a self-assessed approximation score. The commonly used dependent variable is heat-related excess mortality, a statistical estimation, which is used for comparison with aggregated population counts. We observed that self-assessed heat impairment was in agreement with the emotional appraisal of summer heat and the quantity of heat stress symptoms reported by the participants (see section 2.3). Also, we observed similar patterns for risk factors that have already been investigated in previous mortality studies (mainly age and diseases) (Romero-Lankao et al 2012). This agrees with studies that regarded health assessments as top predictors of future mortality, more reliable than physiologic measurements (Mossey and Shapiro 1982, Miilunpalo et al 1997). Ultimately, it indicates general validity of using questionnaires on self-assessed impairment to investigate heat stress risk.
4.2. Risk factors of urban heat stress
The study of vulnerability dimensions revealed that variables related to physical sensitivity returned by far stronger and more numerous associations with heat impairment than the ones related to environmental exposure or adaptive capacity. Our analysis on environmental exposure indicated significant and apparently non-confounded associations for bedroom orientation as individual living space exposure, but no relevant associations for neighborhood exposure.
Physical sensitivity: health and fitness most important
Our main result is that health and fitness was a major factor of individual heat stress risk. First, we observed the strongest statistical correlation with heat impairment for several health and fitness concepts. We found that almost all variables related to health/fitness returned relatively strong and highly significant correlations. Second, we did not find associations of these variables with variables related to exposure or adaptive capacity, even though we investigated a very large set of other variables. Finally, this main outcome is confirmed by earlier laboratory studies that indicated the importance of humans' cardiovascular capacity to compensate elevated body temperature and to mitigate urban heat stress (Kenney and Munce 2003, Kenny et al 2010). We therefore conceive humans' cardiovascular capacity to be the major underlying effect causing individual heat stress. Our study indicates that physical fitness is a relevant indicator of this latent variable. Except for diseases, however, no studies have previously investigated health and fitness variables. The importance of physical sensitivity appears to be generally underestimated in most publications (e.g. Wilhelmi and Hayden 2010).
Previous research identified age and pre-existing medical conditions (chronic diseases) as the dominant risk factors affecting population vulnerability (Reid et al 2009, Oudin Åström et al 2011, Romero-Lankao et al 2012). Our results support this observation for diseases, as the quantity of reported diseases had the strongest association with heat impairment. For specific diseases, we found the strongest associations for the ones that concern the cardiovascular system (see supplementary material, 1.3). For age, see section 4.3.
The investigation of modes of travel indicated that the amount of cycling or active travel showed relatively strong direct associations with heat impairment and associations with other health/fitness variables. We therefore believe that active travel could be regarded as a preventive measure against heat stress (see section 4.4). According to our results, even the use of (semi-active) public transportation was correlated with reduced BMI. In Berlin, one must walk 300–400 m to the next station on average (SenStadt Berlin 2014) including stairways in many stations. Although 'rates of physical activity and general levels of physical fitness are known to provide protection against heat-related ailments' (Yardley et al 2011), we are not aware of any studies that related such variables with heat stress.
Environmental exposure: relevant for personal living space
Environmental exposure has mainly been studied via neighborhood-level urban green spaces, population and building density, in comparisons with heat-related excess mortality. The findings of such studies have been inconsistent (Hajat and Kosatky 2010, Romero-Lankao et al 2012, Harlan et al 2013). Our survey approach allowed for the investigation of personal living space exposure, a more direct exposure concept that cannot be examined at the scale of mortality studies.
Bedroom window orientation in a south-westerly direction appeared as the most relevant risk factor with regard to environmental exposure. This relationship seems plausible, since the solar radiation uptake in south-western oriented rooms is strong just before night time. In our opinion this provides a new and relevant exposure category in heat stress research. Building type and story may be seen as (weaker) risk factors; however, further research is needed to investigate these aspects in greater detail (see supplementary material, part 1). The neighborhood environment, i.e. urban green areas, is known to affect the distribution of land surface temperatures (Dugord et al 2014). However, we did not find significant associations between place of residence and heat impairment. We suggest as possible explanation for this observation that variations in neighborhood environment temperature affect individual heat impairment too indirectly.
Adaptive capacity: low relevance and difficult to assess
Adaptive capacity has been investigated mainly in terms of socioeconomic indicators and social capital (Hajat et al 2007, Uejio et al 2011, Hondula et al 2012). Besides such resource-related indicators of adaptive capacity, our dataset allowed to investigate the effects of heat risk awareness, knowledge and application of adaptation measures.
In contrast to several mortality studies (Medina-Ramón et al 2006, Uejio et al 2011), we did not find strong associations between heat impairment and any of the commonly used socio-demographic variables. Household size was the only clear adaptive capacity risk factor regarding social capital. For other variables, the strong association with age makes interpretation difficult.
4.3. What about age?
Age is widely considered to have a major (direct) effect on heat vulnerability (Oudin Åström et al 2011, Romero-Lankao et al 2012), even though some mortality studies did not find clear associations with age (O'Neill et al 2003, Xu et al 2013).
Our dataset also showed that age had an association of high statistical significance with heat impairment. Yet, the association was not as strong as for health/fitness variables and we observed diverging impairment patterns with increasing age (figure 4). We assume that males in their early seventies that reported strong impairment could be the ones that die earlier as a result of weak physical constitution, confirming the assumption of premature death of the weakest in terms of health capital (Robine et al 2012).
There is evidence from laboratory-based physiological studies that the elderly may have decreased thermoregulation capacities due to decreased blood circulation, and reduced thirst and sweating capacity (Kenney and Munce 2003, Kenny et al 2010). However, this applies only to the elderly at the end of their lives. More generally, when people age, the reduced heat tolerance is believed to be mainly caused by a decrease in aerobic fitness that often, but not necessarily, accompanies aging (Hajat and Kosatky 2010, Kenny et al 2010). 'In fact, studies that have attempted to separate the effects of chronological age from concurrent factors, such as fitness level, body composition, and the effects of chronic disease, have shown that thermal tolerance appears to be minimally compromised by age.' (Kenney and Munce 2003).
Our study provides first empirical findings based on an individual-level survey suggesting that health and fitness could be just as linked to heat stress than age is. Supported by existing knowledge from laboratory studies we believe that physical sensitivity is primarily determined by health and fitness, not by age. While age may still serve as a sound statistical indicator, decision makers should not focus on age in the development of adaptation strategies (see the following section).
4.4. Implications for alternative adaptation strategies
Adaptation strategies lack sufficient empirical evidence on heat stress risk as a fundament and respective policy development seems to be underdeveloped (Kinney et al 2008, Lesnikowski et al 2011, Yardley et al 2011, Wolf et al 2014). Previous recommendations on heat stress adaptation mainly focused on (a) heat exposure reduction via changes in the urban structure (e.g. urban green) or (b) managing health risks through improved heat warning systems and emergency response planning (Wilhelmi and Hayden 2010, Huang et al 2013). Measures that target (a) may reduce people's actual heat exposure, without affecting the important sensitivity dimension. Measures that target (b) deal with symptoms only, but do not tackle any root cause.
Health and fitness has obvious adaptation potential, unlike other recognized risk factors like age. Adaptation could aim at improving population health behavior as a preventive and sustainable adaptation strategy. Adaptation through health prevention, however, is not included in official recommendations at all (EEA 2012, IPCC 2014). This might be a consequence of the perception of urbanization, global warming, and aging as root causes (Fernandez and Creutzig 2015) with limited adaptation potential.
Active travel (walking, cycling) could be a preventive measure (to be started in absence of a heat wave). This has been mentioned by only very few authors (Harlan and Ruddell 2011, Huang et al 2013), but never studied before. Active travel represents the most effective way to improve cardiovascular health by integrating physical activity into daily life routines (Bassuk and Manson 2005, Mackett and Brown 2011, Nazelle et al 2011, WHO 2002, Creutzig et al 2012). And it is already identified as a means for climate change mitigation (EEA 2009, IPCC 2014). Through reduced CO2 emissions from urban transport, societies could reap double rewards by addressing two root causes of urban heat stress: population health and global warming.
A preventive solution in the exposure domain could be the consideration of solar heating effects induced by bedroom window orientations in building design. Heat sensitive people could be advised to avoid unfavorable bedroom orientations. For emergency response, bedroom heat exposure could be reduced for particularly vulnerable people, e.g. those in hospitals (table 1).
Table 1. Major factors of individual risk and potential adaptation strategies.
| Dimension | Risk factors | Adaptation strategies |
|---|---|---|
| Physical sensitivity | Health and fitness major factors of individual risk. Age mostly indirect effect of health and fitness. | Focus on improving population health. Encourage active travel as the most effective prevention strategy. |
| Environmental exposure | Individual living space, in particular bedroom orientation. Neighborhood environment no risk factor. | Advice citizens with low fitness to avoid south-west oriented bedrooms. Provide bedroom cooling for diseased citizens. |
| Adaptive capacity | Risk factor associations less distinct. Socio-economic conditions no risk factor. | Guide citizen awareness from emergency response to long-term preventive measures. |
4.5. Limitations and generalization
The survey design enabled the exploration of a massive set of potential risk factors using descriptive statistics. Variable types and interdependence limited the use of statistical rigorous models and we cannot exclude selection bias from the non-probabilistic survey conducted. However, there were actually striking similarities between the characteristics of our sample and the Berlin population, even though it was not our aim to find representative statistics from our sample. The similarity was not only for the general characteristics of the sample (age, income, gender) but also for the heat-stress relevant characteristics identified in our study (distribution of age, obesity, chronic diseases, household sizes, mobility behavior, etc) (see supplementary material, part 3). Therefore, we assume no relevant selection bias in our survey, for the purpose of this study.
Further, more extensive survey designs could build upon this explorative study to validate the hypotheses it generated. Larger surveys, probabilistic sampling designs, and subsequent more rigorous statistical approaches would allow for a more precise quantification of effect magnitudes and potential confounding effects and to establish functional relationships, e.g. for specific types of diseases or air pollution. The cross-sectional nature of our survey has limitations regarding causal interpretations that could be reduced by longitudinal survey designs. To analyze specific risk factor associations in greater detail, the survey design could be thematically focused, eventually using fully standardized designs.
There are limitations concerning the comparability with mortality studies. However, as discussed in section 4.1, we assume that self-assessed heat impairment and heat-related mortality studies yield similar risk factor patterns, since subjective health indicators are regarded as reliable predictors of future mortality (Mossey and Shapiro 1982, Miilunpalo et al 1997). The question of geographic transfer is also critical. Further research is needed to validate our results and understand prospects for generalizing our main findings by transferring the approach to other cities worldwide.
5. Conclusions
The increasing risk of heat stress represents a major direct consequence of climate change for urban populations. We aimed at investigating urban heat stress risk on the level of individuals to go beyond existing knowledge from mortality studies. We used an observational survey to explore a large set of potential risk factors corresponding to the vulnerability dimensions of physical sensitivity, environmental exposure, and adaptive capacity.
To our knowledge, this investigation is the first of its kind to explore risk factors towards urban heat stress using an extensive individual-level survey. It is a first step towards filling the gap in the literature on how people actually respond to heat stress. It allows for the investigation of new relationships, especially between health/fitness and urban heat stress. Observational social science studies are imperfect due to unquantifiable biases. However, they represent the best possible quantitative methodology. We see enough evidence from our exploratory survey to generate new scientific hypotheses that could be more closely explored in future research.
Our primary hypothesis is that physical sensitivity appears to be the dominant risk dimension, and that it is mainly determined by health status and physical fitness. It is possibly even more important than age per se, the most commonly used risk factor. We cannot see this connection in the frequently employed mortality studies since they simply cannot use health and fitness data. But we can see this link in previous laboratory studies. Indeed, this may all be related to cardiovascular capacity as the underlying causal factor.
Health and fitness has adaptation potential, unlike other risk factors like age. Thus, this could be an avenue for heat stress adaptation. Our results also provided first indication that active travel could be associated with reduced heat stress. Therefore, we suggest that encouraging active travel could be an effective adaptation strategy. In the context of climate change it could serve both for climate change mitigation and adaptation efforts. Bedroom orientation was the only clear exposure effect, which in our opinion could provide another new and relevant exposure category.
Our study provides very interesting findings, useful new insights, and new hypotheses that should be considered in future research work. Our study provides a useful step forward from mortality studies and a starting point for future research in many ways. It emphasizes the value of individual-level survey designs to further close this gap between frequent mortality studies, as commonly employed in the research community, and few laboratory studies.
Further research is needed using extended quantitative surveys to validate our findings and understand prospects for generalizing our main findings. Future research should consider the importance of health and fitness and use such data whenever possible. Then, future perspectives on population risk could be adapted accordingly, by shifting the focus from aging (and urban green) to health and fitness as a root cause, alongside urbanization and global warming. Such a change would allow for preventive policy intervention by improving populations' cardiovascular health.
Acknowledgments
The study was part of the Research Unit 1736 'Urban Climate and Heat Stress in mid-latitude cities in view of climate change' (www.UCaHS.org), funded by the German Research Foundation (DFG) (LA 2525/2-1; 595166). The authors are very grateful to all survey participants for their commitment. We thank Juliane Schicketanz, Christine Wallis, and Sarah Osenberg for their contributions to survey organization and documentation. We thank the courier service Spinning Wheelz and many colleagues for helping to distribute the survey. Special thanks go to Max Schneider and Manfred Leiske for sharing their deep expertise in statistics. We thank several internal (UCaHS research unit) and external experts and colleagues for fruitful discussions.