

Abstract
The risk of radiation effects in children of individuals exposed to ionising radiation remains an ongoing concern for aged veterans of the British nuclear testing programme. The genetic and cytogenetic family trio (GCFT) study is the first study to obtain blood samples from a group of British nuclear test veterans and their families for the purposes of identifying genetic alterations in offspring as a consequence of historical paternal exposure to ionising radiation. In this report, we describe the processes for recruitment and sampling, and provide a general description of the study population recruited. In total, blood samples were received from 91 (49 test and 42 control) families representing veteran servicemen from the army, Royal Air Force and Royal Navy. This translated to an overall response rate of 14% (49/353) for test veterans and 4% (42/992) for control veterans (excluding responders known to be ineligible). Due to the lack of dose information available, test veterans were allocated to a three-point exposure rank. Thirty (61%) test veterans were ranked in the lower group. Nineteen (39%) of the 49 test veterans were classified in the mid (5 veterans; 10%)/high (14 veterans; 29%) exposure ranks and included 12 veterans previously identified as belonging to the special groups or listed in health physics documents. An increased number of test veteran families (20%), compared with control families (5%), self-reported offspring with congenital abnormalities (p = 0.03). Whether this observation in this small group is reflective of the entire UK test veteran cohort or whether it is selection bias requires further work. The cohort described here represent an important and unique family trio grouping whose participation is enabling genetic studies, as part of the GCFT study, to be carried out. The outcomes of these studies will be published elsewhere. ISRCTN Registry: 17461668.
Export citation and abstract BibTeX RIS

Original content from this work may be used under the terms of the Creative Commons Attribution 4.0 license. Any further distribution of this work must maintain attribution to the author(s) and the title of the work, journal citation and DOI.
1. Introduction
The adverse consequences of ionising radiation exposure in utero are known but the heritable effects of parental radiation exposure pre-conception in humans remains uncertain and controversial [1, 2]. To illustrate this, apart from non-significant trends, no epidemiological study has yet conclusively demonstrated any detrimental health effect in the offspring of parents exposed to radiation prior to conception [1, 3, 4]. At the genetic level, an excess of DNA mutations in children has been reported in some [5–8], but not all studies [9–11], including the most recent whole genome sequence analysis of family trios whose parents were exposed as a consequence of the Chernobyl accident [12]. The International Commission for Radiological Protection estimates the human hereditary risk from parental exposure to radiation to be 0.2% Gy−1; however, as this is based upon extrapolations involving large-scale mouse studies and not observable increases in human hereditary disease, the actual risk may be lower [13]. A population of (potentially) radiation exposed individuals comprises veterans of the British nuclear testing programme; it is estimated that over 20 000 UK servicemen attended at least one test site through the 1950s and 1960s. The question of genetic risk remains an ongoing concern for this aged population, therefore the genetic and cytogenetic family trio (GCFT) study was undertaken to, in part, address this. The GCFT study seeks to examine if there is any cytogenetic evidence of historical radiation exposure in nuclear test veterans and if there is any evidence of an increase in genetic alterations in their adult children; the results of this will be published elsewhere. The purpose of the work presented here is to detail the processes for recruitment and blood sampling of the British nuclear test veterans, and also to provide a general description of the study population recruited.
2. Sources and routes of exposure
2.1. Atmospheric and experimental tests in Australia and the South Pacific
The UK detonated 21 atmospheric devices of varying size [yield, given in equivalent kilotons (kt) of TNT] at sites in Western and South Australia and the South Pacific between October 1952 and September 1958. In addition, around 580 minor or experimental trials were carried out in South Australia between 1953 and 1963 before the fields were cleaned up and closed in 1967 (table 1). These are briefly described to provide context for the potential for exposure to ionising radiation. For more information please see [14–17].
Table 1. UK atmospheric nuclear tests and minor experimental trials in Australia and the South Pacific, 1952–1963.
| Site | Operation | Date | Purpose of operation | Yield of bomb (kt of TNT) |
|---|---|---|---|---|
| Atmospheric tests | ||||
| Montebello Islands | Hurricane | 3 October 1952 | Weapon effects | 25 |
| Emu | Totem 1 | 15 October 1953 | Weapon development | 10 |
| Totem 2 | 27 October 1953 | Weapon development | 8 | |
| Montebello Islands | Mosaic G1 | 16 May 56 | Weapon development | 15 |
| Mosaic G2 | 19 June 1956 | Weapon development | 60 | |
| Maralinga | Buffalo 1 (One Tree) | 27 September 1956 | Test warhead | 15 |
| Buffalo 2 (Marcoo) | 4 October 1956 | Test warhead | 1.5 | |
| Buffalo 3 (Kite) | 11 October 1956 | Gather data | 3 | |
| Buffalo 4 (Breakaway) | 22 October 1956 | Test service weapon | 10 | |
| Maldon Island | Grapple 1 | 15 May 1957 | Test thermonuclear weapons | 300 |
| Grapple 2 | 31 May 1957 | Test thermonuclear weapons | 720 | |
| Grapple 3 | 19 June 1957 | Test thermonuclear weapons | 200 | |
| Maralinga | Antler 1 (Tadje) | 14 September 1957 | Weapon development | 0.93 |
| Antler 2 (Biak) | 24 September 1957 | Weapon development | 5.67 | |
| Antler 3 (Taranak) | 9 October 1957 | Weapon development | 26.6 | |
| Christmas Island | Grapple X | 8 September 1957 | Test thermonuclear weapons | 1800 |
| Grapple Y | 28 April 1958 | Test thermonuclear weapons | 3000 | |
| Grapple Z1 | 22 August 1958 | Test thermonuclear weapons | 24 | |
| Grapple Z2 | 2 September 1958 | Test thermonuclear weapons | 1000 | |
| Grapple Z3 | 11 September 1958 | Test thermonuclear weapons | 800 | |
| Grapple Z4 | 23 September 1958 | Test thermonuclear weapons | 25 | |
| Experimental trials | Number of trials | |||
| Maralinga | Kittens | 1953–1961 | Testing weapon components | 99 |
| Tims | 1955–1963 | Testing weapon components | 321 | |
| Rats | 1956–1960 | Testing weapon components | 125 | |
| Vixen A | 1959–1961 | Dispersal by fire and explosion | 31 | |
| Vixen B | 1960–1963 | Effect of accidental detonation | 12 | |
| Ayres, Hercules, Brumby | 1960–1967 | Clean-up operations | ||
a South Australia. b The first Kittens trials in 1953 took place at Emu.
The first British test, Operation Hurricane, took place off the Montebello Islands with the objective of assessing the effects of atomic weapons, including from the blast and from radiation. This was followed a year later by Totem 1 and 2 which were tower-mounted devices and part of the programme for the early development of weapons. Operation Mosaic (G1 and G2), again both tower-mounted devices, furthered this weapons development and additionally sought to understand the effects of fallout on naval vessels. To this end, HMS Diana was tasked with sailing through the nuclear plume. The first atomic bomb tests to take place on the Maralinga Range, South Australia were part of Operation Buffalo. This test series also represented the first time animals were used to understand the effect of detonations. Additionally, officers known as the Indoctrinee Force were positioned closer to ground zero for purposes of inspecting equipment and to gain insight into nuclear warfare. The Operation Grapple test series, took place in the Pacific Ocean, on Malden Island and Christmas Island (Kiritimati, ∼400 miles north of Malden Island). The first of these (Grapple 1,2,3) included Grapple 1, which was the first thermonuclear device detonated by Britain. Like the other tests in this series, the device was delivered from a Vickers Valiant bomber producing a mushroom cloud rising high into the atmosphere. Grapple 2 followed, which with a yield of 720 kt was a record for a pure fission bomb. By contrast, the last in this series, Grapple 3, only yielded ∼200 kt which was less than expected. Operation Antler on the Maralinga range followed Grapple 3 and had the aim of furthering weapons development. Antler 1 and 2 were both relatively low-yield tower-mounted devices generating clouds rising to ∼3000 m and 7000 m, respectively. Antler 3, detonated from a balloon tethered from the ground, generated a much higher explosive yield although the resulting plume was lower than expected. There followed three additional series also under the operational codename Grapple which took place off Christmas Island in the Pacific Ocean. Grapple X was an airburst yielding 1.8 Mt in explosive power ∼8000 ft above the ocean. This was followed by Grapple Y, the largest ever British nuclear bomb to be tested with a yield of 3 Mt. The final series of four tests, codenamed Grapple Z1–4, were airburst devices carried out to enhance bomb design and minimise premature detonation; these varied in yield from 24 kt to 1 Mt.
The minor trials or experimental programme, which took place principally on the Maralinga range in South Australia between 1953 and 1963, was designed with the aim of understanding aspects of weapon design and safety. The early trials (Kittens, Tims and Rats) focused on the design of individual components of the nuclear device, and the later trials (Vixen) considered transportation and storage safety concerns. Relatively large quantities of radioactive material including Pu-239, U-235, U-238, Po-210 and the element beryllium were dispersed into the surrounding area as a consequence of the Vixen trials and the range was deemed highly contaminated. As part of the closure of the Maralinga site, contaminated debris and soil was buried during clean-up programmes which continued until 1967 (Ayres, Hercules, Brumby; table 1).
2.2. Potential sources and routes of exposure
The potential sources and routes of exposure include: prompt exposure from the initial flash of radiation, exposure from radioactive materials associated with the test and from fallout. Taking these in turn, prompt exposure produced in the first minute after detonation generally comprises a burst of gamma rays and neutrons. The associated dose falls rapidly with distance from the point of detonation whereby by ∼2.5 km the gamma dose is around 10–20 mGy and beyond 5 km the dose is effectively negligible [18]. For the majority of the British tests, service personnel were mustered on beaches around 40 km from blasts, on airfields around 32 km from blasts or on decks on ships which were patrolling outside the blast zone.
The main types of radioactive material of concern are activation products, fission products and unconsumed nuclear fuel. Activation products are generated from neutrons produced in the explosion, which are then absorbed by nonradioactive atoms including dust and equipment in the surrounding area (up to about 1 km), which then become radioactive. Fission products are the hundreds of different radionuclides produced when plutonium or uranium atoms split in the nuclear fission reaction. These may rise with the nuclear plume and disperse into the upper atmosphere and/or deposit more locally around the test (ground zero) zone. Both activation and fission products include a wide array of short- and long-lived radionuclides with declining risk over time according to their half-life, although longer-living radionuclides such as Pu-239 can result in an internal dose which accumulates over a person's lifetime [19–21].
Atmospheric tests release substantial amounts of radioactivity, and much of this goes into the upper atmosphere, contributing to the global levels of radiation before eventually dropping to earth as fallout. Many of the bombs were detonated high in the atmosphere to reduce localised nuclear fallout, with the height to which the radioactive plume rises depending largely on the size and efficiency of the explosion. Fallout includes fission products, activation products and residual unconsumed plutonium and uranium, and subsequent dispersion is mainly determined by weather patterns including rainfall, wind speed, direction and temperature, all of which vary with height [22–24]. Optimal conditions for proceeding with any detonation were defined; however, as noted earlier, for some tests these conditions were not met and/or the expected outcome of explosion in terms of plume height or size were not achieved, meaning the potential for localised fallout may have occurred.
In terms of potential routes of exposure, for external exposure this mainly relates to being in, or moving over, ground or water which is contaminated. Exposure may also occur due to clouds of fission or activation products passing overhead, from flying in aircraft collecting nuclear plume samples or from sailing in ships navigating through contaminated air/waters [19, 25, 26]. In all these instances, exposure will cease when the contaminated area is left, but only if there is no contamination on the vehicles/ships in which personnel are travelling and/or on clothing. This is also relevant for internal exposures whereby radioactive dust in contaminated clothing and equipment can become dislodged and inhaled at later times. Internalised radioactive contamination can result in an internal dose accumulation over a person's lifetime: the extent and potential harmful effects of this depend on the amount internalised, the physical and biological half-life of the radionuclides and associated emission characteristics [21].
2.3. Monitoring of dose and potential for exposure
Dose estimates for British nuclear test veterans are based on film badge measurements of external dose compiled by health physics staff at the Atomic Weapons Research Establishment (AWRE) in the 1960s. Neutron doses were not recorded, while for some operations the dose badges issued had a high minimum threshold of detection meaning smaller doses would not have been recorded. Apart from limited autopsy analysis carried out subsequent to the tests, no measurements of internal dose were made; however, the Ministry of Defence (MoD) acknowledge that undocumented internalisation of radionuclides would have been likely but limited to employees of the AWRE or those attending the minor trials at Maralinga [27]. Accordingly, the uncertainties in estimates of the dose received by some veterans may be large.
The UK nuclear test veteran's cohort was compiled by the National Radiological Protection Board through identification of 22 347 male armedservice personnel and male employees of both the AWRE and Atomic Energy Research Establishment who had participated in the tests [28]. This was reduced to 21 357 in a later analysis [29]. A matched control group of 22 333 armed services personnel who served in the tropics at the same time but who were verified as not present at any test sites were also identified. The cohort was restricted to male servicemen since very few women took part in the tests [14].
According to the health physics records (as noted in Kendal et al [14]), dose was recorded for 21% of the whole cohort, with only 8% recording a non-'zero' radiation dose (zero defined as a reading below the limit of detection) [14]. The majority of this 8% (1635 participants) were sub-classed as having an external dose range of between 0 and 50 mSv for the whole test programme, 44 participants were categorised as receiving between 50 and 100 mSv and 36 as receiving a dose of >100 mSv. Overall, 759 test veterans were categorised into 'special groups'. These included the Buffalo Indoctrinee Force, RAF crews involved in air sampling, RAF active handing flights who decontaminated aircraft, the crew of the HMS Diana who sailed through the plume at Operation Mosaic and the Target Response Group at Buffalo. Estimated doses within the special groups are: (a) the Buffalo Indoctrinee Force (172 individuals with a mean recorded dose of 2.1 mSv), (b) RAF radioactive cloud sampling crew (98 individuals with a mean recorded dose of 84 mSv), (c) RAF active handling flight crew (130 individuals with a mean recorded dose of 4.6 mSv), (d) the crew of HMS Diana (282 individuals; one recorded dose of 0.2 mSv) and (e) the Target Response Group at Buffalo (77 individuals with a mean recorded dose of 8.3 mSv) [14]. Many of those present at test sites were involved in support roles, such as construction, transport or catering, but additionally were directly involved with the actual tests, including working in contaminated areas in the days, weeks and months following each test [29]. Such roles may or may not have been accounted for by the formal categorisation into a special group.
This UK cohort has been previously described and followed through national registration for cancer registration and mortality [14, 27–30]. The most recent update to 2017 reported some evidence of overall increased mortality (relative risk = 1.02, 90% CI 1.00–1.05, p = 0.04), which was associated with increased risks both for all cancers and for non-cancer diseases [31]. To date there have not been any peer-reviewed studies among offspring of the nuclear test veterans. The GCFT study seeks to examine if there is any evidence to support there being a genetic legacy from participation at historical British nuclear test sites. This includes a cytogenetic examination for evidence of historical radiation exposure in nuclear test veterans and cytogenetic and whole genome sequence analysis for the detection of germline mutation. The results will be published elsewhere. The purpose of the work presented here is to detail the processes for recruitment and sampling of the British nuclear test veterans and to provide a general description of the study population recruited.
3. Methods
The aim was to recruit 50 nuclear test veterans born since 1935 (aged ⩽82 years at interview), their wives/partners and one biological child as test veteran trios and 50 veteran trios (veteran, wife/partner and one biological child) who had no history of nuclear test participation as control families.
3.1. Ethical and regulatory approvals
The study was conducted in accordance with UK ethical framework and approved by the UK Health Research Authority (17/LO/0273). Permissions were obtained from the MoD and Public Health England (PHE) to access the 'UK nuclear test veterans' cohort. Further approvals were obtained from the UK Confidentiality Advisory Group, NHS Digital and 15 local clinical research networks in England and seven equivalent health boards in Wales, in order to use this information for the purposes of identifying and inviting individuals to the study. To reduce the number regulatory approvals required, the study was restricted to those registered with a general practitioner (GP) in either England or Wales.
3.2. Recruitment of family trios
Armed services test and control veterans were selected for invitation to participate from the UK nuclear test veteran's cohort [14, 27, 28, 32]. PHE, as custodians of the cohort, were able to provide anonymised basic exposure data (age, special group status and operation name/test/year present at) for 5818 veterans and 6101 control veterans who were aged ⩽82 years and thought to be alive and cancer-free. In order to select the veterans with the highest likelihood of exposure, 1459 case veterans were selected if they were currently aged ⩽80 years and had participated in two or more operations which included the Grapple X, Y, Z series, Maralinga test sites and/or those who had special group status. In addition, a small number (n = 42) of veterans aged ⩽82 years who were part of the crew of HMS Diana, active handling flight or aircrew sampling plumes special groups were also included. NHS Digital provided GP contact details for 908 test and 3796 control veterans from the identifying information provided directly by PHE; all 908 test and 2741 control GPs were contacted with the request to forward invitation packs. From this a total of 405 test veterans and 1028 control veterans, group-matched on age, service [Royal Air Force (RAF), Royal Navy, Army] and period of service in tropical regions, were invited to participate in the study via GP practices (figure 1).
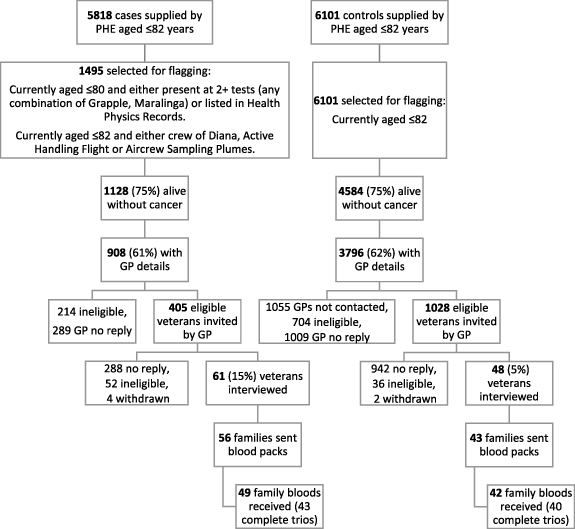
Figure 1. Study flowchart: cohort selection, invitation and response.
Download figure:
Standard image High-resolution image{kind=link}
Participant invitation packs were sent to GPs with a request to confirm study eligibility and, if medically appropriate, to forward the invitation. Responding veteran couples were screened by telephone to confirm eligibility and gain written informed consent. Military service details and other potential clastogenic exposures were also collected from veterans using a structured questionnaire. Consenting couples were asked to share study invitation details with a child they had together and who was conceived after the veteran returned from his last tour at a nuclear test site. For veteran couples with more than one child, participation by the first child to be conceived since the veteran's last tour of duty was requested to minimise potential selection bias. Confirmation of the eligibility of interested offspring respondents was obtained via their GP following a screening telephone call with the child and prior to informed written consent being obtained (figure 1). Veterans and children were excluded from study participation if they were known to have had a previous history of chemotherapy for cancer treatment, cytotoxic chemotherapy (such as methotrexate for rheumatoid arthritis) or radiation treatment for any reason as this could cause genetic damage and interfere with interpretation of the study.
Upon receipt of written consent from each family trio, study packs for sampling whole blood were delivered to the family with a request for their GP to sample and ship to Brunel University London within 24 h, where all samples were stored in compliance with Human Tissue Authority guidance. Lithium heparin blood samples were immediately processed for cytogenetic analysis with isolation of peripheral blood lymphocytes for long-term storage where possible and EDTA tubes were stored for batch shipment to the University of Leicester where they were sequenced using whole genome sequence techniques [12, 33–36]. The results of this analysis will be reported elsewhere.
3.3. Radiation exposure
The process of verifying participation at nuclear test sites and inclusion into the UK nuclear test veterans cohort have been described [14, 32]. In this study, further verification was carried out revealing very few discrepancies between the details (dates and tests) obtained from the telephone interview and PHE records.
The majority of test veterans in the UK nuclear test veterans cohort have no recorded dose as only a limited number were issued with film badges, mainly accounting for those identified in special groups, and no measurement for internal contamination took place. Based on the testimony and verified operation attendance and, blind to any results, the test veterans were assigned to a three-point rank for the potential of internal/external exposure (table 2). Each case was a priori assumed to be in the lowest rank, and a higher rank was allocated only if sufficient information was given to suggest a higher likelihood for radiation exposure. A defined role in a contaminated or forward area (e.g. aircraft sample retrieval/cleaning) undertaken more than once was considered to have a higher exposure potential, and here we distinguished between activities immediately and up to 3 months after the test where dose and dose rates would be expected to be highest (higher rank) or at any time from at least 3 months after the test (medium rank).
Table 2. Exposure ranking definition.
| Potential for radiation exposure | Rank group | |
|---|---|---|
| Background | Control veterans not present at test sites | 0 |
| Lower | Equivalent to observation from safety zones OR in the vicinity for ∼12 months | 1 |
| Medium | Defined role (more than once) in forward/contaminated area (including aircraft sampling retrieval/cleaning) >3 months after test | 2 |
| Higher | Defined role (more than once) in forward/contaminated area (including aircraft sample retrieval/cleaning) within days/weeks after test | 3 |
4. Results
4.1. Response rates
A total of 3649 invitation packs (908 test veterans and 2741 veteran controls) were sent to GPs in batches from October 2017 to July 2019. Of these, 918 veterans (23.6% test and 25.7% control) were deemed by GPs as ineligible (46% of these had no surviving wife/partner or child). No GP response was received for a further 1298 veterans (31.8% test and 36.8% control), while the remaining GPs forwarded invitations to 1433 veteran couples (44.6% test and 37.5% control). Of the 1433 invitation packs forwarded to veteran couples, 117/405 (29%) test and 86/1028 (8%) control couples returned the reply slip. A further 87 of these were deemed to be ineligible, mostly because they had no surviving wife or children, which left 115 (65 test and 50 control) eligible couples, of whom 112 (63 test and 49 control) consented. Of the 112 consenting couples, 100 full family trios consented to take part in the study (57 test and 43 control), with blood samples received from 91 (49 test and 42 control) families between February 2018 and February 2020. Of these, full blood trios were received for 43 test and 40 control families as six test and two control families had either no child or mother blood sample, mainly due to difficulties in sampling arrangements, including Covid-19 restrictions (figure 1). The overall response rates for veterans providing a blood sample were 13.9% (49/353) for test veterans and 4.2% (42/992) for control veterans (denominators are taken as number invited excluding those known to be ineligible).
4.2. Age
The test and control veterans were similarly matched with a median year of birth of 1938 (ranging from 1936–1944 for test veterans and 1935–1942 for controls) and hence a median age (when blood was taken) of 80 years (ranging from 74–83 years for test veterans and 76–83 years for controls). The median age of their partners was 77 years for both test veterans and controls (ranging from 61–86 years for test veterans and 63–87 years for controls) and 53 years for the children of test veterans (range 27–59 years) and 52 years for children of controls (range 38–60 years). The median interval from exposure to conception among the test veterans and their child was 5 years (49% 0–4 years, 31% 5–9 years and 20% >10 years).
Table 3 shows a similar distribution between the test and control participants by service and age at blood sampling. Both test veterans and controls joined the services in 1956 on average (range 1951–1960), although the controls tended to remain in the services for longer (45% remaining in the services for 10 or more years compared with 29% of test veterans). Most of the control veterans were stationed in Malaysia/Singapore (50%) and Yemen/Persian Gulf (24%) with the remainder in Hong Kong (9%), Sri Lanka (5%), the Pacific (5%), Australia (5%) and the Caribbean (2%).
Table 3. Veterans by age at blood test and service.
| Age at blood sample (years) | Army | RAF | Royal Navy | Total | ||||
|---|---|---|---|---|---|---|---|---|
| Control | Test | Control | Test | Control | Test | Control | Test | |
| 74–80 | 6 | 12 | 9 | 8 | 6 | 6 | 21 | 26 |
| 81–83 | 11 | 10 | 8 | 8 | 2 | 5 | 21 | 23 |
| Total | 17 | 22 | 17 | 16 | 8 | 11 | 42 | 49 |
4.3. Service history of test veterans
Test veterans were selected according to likely exposure based on the limited information within the PHE records. Supplementary table 1 (available online at stacks.iop.org/JRP/42/021528/mmedia) shows these exposure data (number of operations, member of special groups or listed in health physics) for the 1495 cases selected, the 908 invited and the 49 who provided blood samples. Twelve (25%) of the test veterans taking part were members of the special groups or listed in health physics, similar to the proportion (27%) in the cohort overall.
The majority of test veterans recruited were stationed at Christmas Island (57%) with the remainder at Maralinga (35%) or Montebello (8%). The four men in the Royal Navy who were present at Montebello were all ranked in the higher exposure group. Three were crew of HMS Diana (special groups) and the other was listed in health physics records. Half of the men present at Maralinga and a quarter of the men present at Christmas Island were ranked in the mid or higher exposure groups (table 4). Overall, 30 (61%) of test veterans were ranked in the lower group, 5 (10%) in the mid group and 14 (29%) in the higher exposure group.
Table 4. Number of men present at test sites by exposure ranking and service.
| Exposure ranking | Service | ||||||
|---|---|---|---|---|---|---|---|
| Test site | n | Lower | Mid | Higher | Army | RAF | Royal Navy |
| Montebello–Mosaic (1956) | 4 | 0 | 0 | 4 | 0 | 0 | 4 |
| Maralinga (1957–1963) | 18 | 9 | 4 | 5 | 10 | 3 | 5 |
| Christmas Island (1957–1958) | 29 | 22 | 1 | 6 | 12 | 13 | 4 |
| All case veterans | 49 | 30 | 5 | 14 | 22 | 16 | 11 |
a One serviceman spent time at both Maralinga and Christmas Island and one spent time at Montebello and Christmas Island. b Six veterans were present at Antler (1957) and 17 were present during the experimental programme (1953–1963) including five who were present for both. c All but one serviceman was present at Grapple Y (21 men) and/or Grapple Z (26 men). Seven men were also present for Grapple X and two men were present for Grapple 1, 2, 3.
4.4. Other hazardous exposures
Table 5 shows other exposures recorded from the structured interview by test and control veterans. Higher proportions of control veterans reported occupational chemical or radiation exposure (p = 0.02), but similar proportions of test and control veterans reported ever smoking, drinking alcohol regularly, having x-rays, CT scans or other scans involving radiation.
Table 5. Other exposures reported by test and controls.
| All veterans | ||||
|---|---|---|---|---|
| Controls | Test | |||
| n | % | n | % | |
| Occupational chemical exposure | 32 | 76.2 | 26 | 53.1 |
| Occupational radiation exposure | 18 | 42.9 | 10 | 20.4 |
| Ever smoked | 30 | 71.4 | 37 | 75.5 |
| Regularly drinks alcohol (⩾14 units per week) | 22 | 52.4 | 28 | 57.1 |
| Number of x-rays | ||||
| None | 0 | 0 | 2 | 4.1 |
| 1–4 | 19 | 45.2 | 19 | 38.8 |
| 5–9 | 11 | 26.2 | 15 | 30.6 |
| 10+ | 12 | 28.6 | 13 | 26.5 |
| Ever had a CT scan | 23 | 54.8 | 30 | 61.2 |
| Ever had other type of scan | 18 | 42.9 | 27 | 55.1 |
| Total | 42 | 49 | ||
a Worked in nuclear industry or possibly exposed to radiation during their occupation. Only two test and two control veterans were likely to have episodes of radiation exposure above a 'safe/usual' level.
4.5. Reported diseases or disorders
During the interview, the veterans were asked whether they were aware of any birth defects, genetic disorders, inherited diseases or cancers that had affected their children or grandchildren. These were coded blind to test–control status to exclude any with evidence of being familial (table 6). A fifth of the test veterans reported a congenital abnormality among at least one of their children or grandchildren, this included two who were stillborn, which was higher than the small number reported by the control families (Fisher's exact p = 0.03). There was no evidence in this small study of any increased rates of cancer or other diseases among children (average age 53 years) of the test veterans (Fisher's exact p = 0.19 and p = 0.6). Of the 6 control and 17 test families in table 6 reporting at least one disorder/disease in the family, only two control and five test families provided blood samples for the affected child. (The protocol was to ask the oldest child conceived after the last tour in the South Pacific to provide a blood sample.)
Table 6. Self-reported congenital abnormalities, cancers and other non-familial disease affecting any child or grandchild of the veteran.
| Control, n (%) | Test, n (%) | |
|---|---|---|
| Congenital abnormality | 2 (4.8%) | 10 (20.4%) |
| Cancer | 2 (4.8%) | 6 (12.2%) |
| Other non-cancer diseases | 2 (4.8%) | 4 (8.2%) |
| Any disease/disorder | 6 (14.3%) | 17 (34.7%) |
a Families are counted once in each row. Three test families reported congenital abnormalities plus one other disease group: two families reported cancers in a second family member, and one family reported both congenital abnormality and another disease within the same child. b In addition to the families in a, one family reported several congenital abnormalities in several family members.
5. Discussion
The GCFT study is the first study to obtain blood samples from a group of British nuclear test veterans and their families for the purposes of identifying genetic alterations in offspring as a consequence of historical paternal exposure to ionising radiation. The study is designed to ask firstly if there is any cytogenetic evidence of historical exposure to ionising radiation in veterans of the testing programme. For this, 24-colour karyotyping (multiplex fluorescence in situ hybridisation (M-FISH)) is being used to detect the occurrence of stable and unstable chromosome exchanges of varying complexity [35]. Accordingly, aberrations that have persisted over time and those that may be more recently induced, arising as a consequence of lifestyle/medical/occupational factors, ongoing internalised exposure or through other mechanisms including delayed genomic instability, may be compared between the test and control veterans groups. Secondly, we are asking if there is any evidence of chromosomal or DNA alterations in the children of British nuclear test veterans. Here we are employing G-band analysis to determine the chromosome constitution that adult children were born with and, additionally, Giemsa block staining to look for evidence of genomic instability. Finally, the GCFT study is using whole genome sequence techniques to examine for the occurrence of newly arising germline mutations including single nucleotide variants, small insertions–deletions, structural variants or clustered mutations. The findings pertaining to these questions will be reported elsewhere. In this report, we describe the methodology and the population recruited to the GCFT study. In total, blood samples were received from 91 (49 test veterans and 42 controls) families representing veteran servicemen from the army, RAF and Royal Navy. Nineteen (39%) of the 49 test veterans were classified in the mid/high exposure rank and included 13 veterans previously identified by PHE as belonging to the special groups or listed in health physics documents.
The requirement to obtain blood samples from entire family trios (three family members) limited the recruitment of this already aged population where the veterans were aged 80 years on average [37]. We were required by the Data Protection Act to invite individuals via their GP practice, which precluded verification of the initial participant invitation as well as the possibility of sending a reminder. The majority of veterans did not reply to the invitation (71% of test veterans and 92% of control veterans) and the proportion of ineligible non-responders was not known. Further to this, the lengthy multi-step nature of recruiting entire family trios (couple GP verification, invitation, screening and consent followed by child invitation via parents, child GP verification, screening and consent and finally blood samples) further reduced the overall trio response rate. Overall, 14% of test and 4% of control families provided at least one blood sample. The Covid-19 pandemic halted recruitment in March 2020, but blood samples were received for 49 case and 42 control veterans (6 test and 2 control families were not complete trios).
Despite the measures taken to reduce bias in the recruitment methods, the recruitment rates for providing blood samples were low and so it is possible that those taking part had a particular interest in the study. The test veterans may have been more likely to take part if they believed they had been highly exposed to radiation during the tests or that their family had been adversely affected. Ten of the 49 test veterans (20%) reported at least one congenital abnormality among their children or grandchildren, which is higher than that reported by control families (2; 5%) (p = 0.03) and in the general population (∼2%) [38]. We may have seen this difference because there is a higher rate of congenital abnormality among the offspring of exposed veterans and this would be a likely explanation if the test and controls recruited to our study are largely representative of the entire cohort of UK nuclear test veterans. If, however, the test veterans were more likely to take part in our study if they believed their family to be adversely affected, the higher rate of congenital abnormality would be due to selection bias. No hereditary effects have been detected among those conceived after one or both parents were exposed to the atomic bombs in Japan during World War II, which is the largest intergenerational study to examine health outcomes [39]. That said, the only unbiased way to answer this question is to link families and systematically search medical records, which would be challenging now in the UK. Blood samples were requested where possible from the first child conceived after last test attendance, and therefore only two of the ten families reporting congenital abnormality within their family provided blood samples for the child with the abnormality.
We observed a higher proportion of control veterans (n = 18, 43%) reporting occupational exposure to radiation than among test veterans (n = 10, 20%); however, only two test veterans and two controls reported exposure which may have been of relevance (three of four outside their military careers). Remaining exposures included working with radar equipment which can emit parasitic x-rays (bremsstrahlung; six controls and three test veterans) or being in the vicinity of nuclear establishments/devices, and most of these (16/24) occurred during their military careers. Control veterans had longer military careers than the test veterans, which may explain their higher number of reported exposures. Again, it could be that longer-serving control veterans, or those exposed to radiation at other points in their careers, may be more interested in our study and were more likely to take part.
Responders to epidemiological studies are usually healthier and more educated than the general population [40]; however we found no difference in the distribution of indices of deprivation linked to the postcode of the GP surgery of the veterans who took part in the study compared with those who did not respond (data not shown). It could be that the UK nuclear test veteran controls are all ex-military and therefore more homogeneous. Given the concerns over selection bias (higher frequency of congenital abnormalities among children of test veterans and higher frequency of other occupational radiation exposure among the controls), comparisons between the testimonies from test veterans and controls should be regarded with caution. Any selection biases which may exist, however, should not affect the cytogenetic analysis or germline results, particularly if a proxy dose–response relationship is seen with exposure variables.
Only 7% of the PHE cohort had recorded dose information, yet testimony from veterans in the public domain highlighted concerns that exposure was not limited to just those issued with film badges. Accordingly, in this study, selection included those with no record of dose but whose potential for exposure was increased through attendance at multiple operations and special group status. The scant military record provided by PHE pertaining to this, i.e. a list of tests and membership of special groups, was close to the testimony taken by telephone interview.
The a priori exposure ranking was done blind to any results and therefore is an unbiased assessment of potential for exposure. About a third of the men aged ⩽80 years on the PHE file were selected for flagging by NHS Digital based on the criteria of belonging to a special exposure group and/or present at two or more tests including Grapple or Maralinga. All 405 test veterans identified as eligible by GPs were invited to take part. Despite this initial selection for invitation, 30/49 of test veterans recruited were categorised into the lowest exposure rank based on their testimony, as most veterans reported observing the tests from the safety zone. A higher exposure ranking was associated with being present at Montebello or Maralinga rather than the later tests at Christmas Island. Cleaning aircraft and supporting sample collection were activities that were also associated with the higher ranking, mainly due to the potential for internal exposure from breathing in dust generated by the actual trials or stirred up by working in contaminated areas. Testimony on consumption of contaminated foodstuffs was limited, but any contribution of dose from eating or drinking is likely to be less [19, 22].
In summary, we present here the family trios recruited to take part in the GCFT study. All services of the armed forces are represented with nuclear test and control veterans groups matched on age and service. The recruitment rate was low, and although this was anticipated due to the advanced age of veterans and the need to recruit family trios, it may have resulted in bias related to reasons for participating. These include those who were motivated to participate (both nuclear test and control veterans) due to concerns about exposure during the tests or to occupational sources of radiation and/or the health of family members. Our methodological approach of inviting veterans to participate based upon our selection from the UK cohort would reduce this bias but not exclude it. Accordingly, the finding of an increase in congenital conditions in the families of nuclear test veterans should serve as a basis for further investigation.
Acknowledgments
We are grateful to and thank all families for their participation in and support of this project. We acknowledge support from PHE (UK HSA) for access to the UK nuclear test veterans cohort. Our thanks also extend to Professor Dudley Goodhead OBE, Dr Mark Hill and Professor Mark Pearce for their useful comments on this manuscript and Ms Emily Al-Haddad for her clerical assistance.
Funding
This work was supported by the Nuclear Community Charity Fund (NCCF) through funds received by The Armed Forces Covenant Fund Trust under the Aged Veterans Fund Grant AVF16 and Brunel University London under Grant 10790100.