

Abstract
Fixed-beam radiotherapy systems with subjects rotating about a longitudinal (horizontal) axis are subject to gravity-induced motion. Limited reports on the degree of this motion, and any deformation, has been reported previously. The purpose of this study is to quantify the degree of anatomical motion caused by rotating a subject around a longitudinal axis, using cone-beam CT (CBCT).
In the current study, a purpose-made longitudinal rotating was aligned to a Varian TrueBeam kV imaging system. CBCT images of three live rabbits were acquired at fixed rotational offsets of the cradle. Rigid and deformable image registrations back to the original position were used to quantify the motion experienced by the subjects under rotation.
In the rotation offset CBCTs, the mean magnitude of rigid translations was 5.7 ± 2.7 mm across all rabbits and all rotations. The translation motion was reproducible between multiple rotations within 2.1 mm, 1.1 mm, and 2.8 mm difference for rabbit 1, 2, and 3, respectively. The magnitude of the mean and absolute maximum deformation vectors were 0.2 ± 0.1 mm and 5.4 ± 2.0 mm respectively, indicating small residual deformations after rigid registration. In the non-rotated rabbit 4DCBCT, respiratory diaphragm motion up to 5 mm was observed, and the variation in respiratory motion as measured from a series of 4DCBCT scans acquired at each rotation position was small.
The principle motion of the rotated subjects was rigid translational motion. The deformation of the anatomy under rotation was found to be similar in scale to normal respiratory motion. This indicates imaging and treatment of rotated subjects with fixed-beam systems can use rigid registration as the primary mode of motion estimation. While the scaling of deformation from rabbits to humans is uncertain, these proof-of-principle results indicate promise for fixed-beam treatment systems.
Export citation and abstract BibTeX RIS
1. Introduction
The standard approach to radiotherapy has been for the imaging and treatment beams to be on a gantry rotating about a patient receiving treatment on a fixed couch. Fixed-beam systems would lower the cost of particle therapy (Burns and Potts 1992, Pankuch 2015), MRI-guided and economical photon linacs (Eslick and Keall 2015, Feain et al 2016, 2017b). However, patient rotation would be required to provide multi-field and arc deliveries equivalent to modern treatment deliveries on rotating gantry equipment (image-guided modulated treatments with passive respiratory motion management).
Image-guided small animal irradiator prototypes have been used with fixed kV sources and rotating subject stages, with the animal cranial-caudal axis placed vertically (Wong et al 2008, Matinfar et al 2009). To scale up to human treatments, the vertical patient orientation would have limited applications due to restricted beam geometry when seated or inability to maintain an upright weight bearing position over treatment. For a fixed-beam treatment system that could be used on all patients, the ideal configuration would be to have the patient lay down and rotate on a longitudinal axis, as this allows beam paths to most anatomy and would match standard simulation CT images and experience. Longitudinal rotation would introduce anatomic structure movement of the patient due to gravity as the couch support system rotates, which is a challenge for accurately conforming the treatment beam to the desired targets and minimising healthy tissue irradiation.
This investigation was performed to determine the feasibility of treatment units with fixed-beam and longitudinal subject rotation. Such a system would need to account for any motion created by subject rotation, in both treatment and image guidance systems. Modelling gravity effects on the pose of an external structure is a prominent issue in computer vision, incorporating articulated body pose estimation and pose space deformation (Lewis et al 2000). However, to date there has been little work to assess internal anatomical deformation.
The purpose of this study is to quantify the degree of anatomical motion caused by rotating a subject around a longitudinal axis, using cone-beam CT (CBCT). Respiration is the main source of motion in a non-rotated patient, and the gravity-induced deformation is compared to nominal respiratory deformation of the subject using 4DCBCT. This is the first study of CBCT imaging of live subjects undergoing gravity-induced motion, and as such it is piloted on small animals.
2. Methods
2.1. Image acquisition
A purpose-built rotating immobilization cradle was positioned on the couch system at isocentre of a Varian TrueBeam linac v2.5 (Varian Medical Systems, Palo Alto CA), and its longitudinal rotation axis aligned to rotational axis of the gantry. This cradle acts as a simplified miniature of the couch in Feain et al (2017a). CBCT images of the cradle at fixed rotation offset increments were used to ensure the alignment and concentricity of the cradle and the linac imaging system.
In an institution ethics committee approved study (University of Sydney Animal Ethics Project 2015/903), three New Zealand white rabbits of 12–16 weeks (weighing 351, 359 g and 406 g; caudal-cranial lengths approximately 22 cm) were imaged under free-breathing. Rabbits were placed in the cradle in the standard anatomical position (see figures 1 and 2). The rabbits were immobilised in the rotation cradle using adjustable straps, packed with bubble-wrap and secured in a wrapped towel. The cradle allowed 360° positioning under computer control. A veterinary surgeon anaesthetised each animal prior to imaging, and monitored them throughout the experiment.
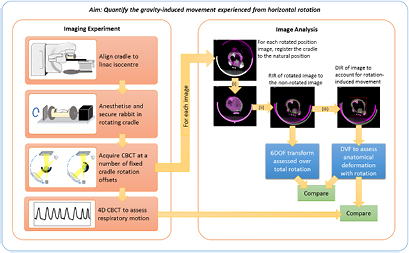
Figure 1. Study design overview. The cradle in the zero offset (non-rotated) position. Rabbits were placed within the tube cutaway, and secured with adjustable straps and bubble-wrap packing (not shown). CBCT were then acquired at fixed rotation offset increments over a full revolution. All images were registered with both rigid and deformable methods to the zero offset position, to quantify movement due to the applied rotations. RIR = rigid image registration. DIR = deformable image registration.
Download figure:
Standard image High-resolution image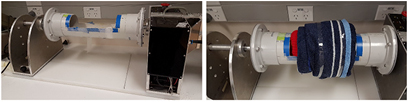
Figure 2. Left picture shows rotation cradle with cutaway section for securing the subject, which resides on a flat wax base inside the tube cradle. Motor and computer control for rotation is in rear. Right is a mock-up immobilisation of a subject. The cutaway section is packed with bubble wrap, and secured around the subject with towel padding, ensuring adequate ventilation.
Download figure:
Standard image High-resolution imageEach rabbit was imaged with the following standard series: (1) An initial slow CBCT for 4DCBCT reconstruction with the cradle level and rabbit in standard anatomical position ('zero increment'). Images were based on the Head pre-set, with reduced gantry speed; (2) A series of standard CBCT (standard Head pre-set) with rotating gantry were acquired with the cradle rotated to a fixed position (this position will be referred to as the 'fixed increment', and typically increment by 45° between image series). This was repeated over two full revolutions of the cradle, resulting in 16 CBCT. Additional series were acquired during another revolution which varied for each subject. These were: test of reproducibility and repeated rotations (rabbit 1), assessing gravity-induced changes to respiratory motion (rabbit 2) and assessing gravity-induced motion with finer resolution using smaller fixed-increment size (rabbit 3). The complete imaging schedule is detailed in table 1. Continuous fluoroscopy with a fixed gantry position and constantly rotating cradle was acquired for a complementary project looking at reconstruction incorporating gravity-induced deformations (Shieh et al 2017). The settings for each acquisition are given in table 2. All reconstructions used standard settings for the Head pre-set.
Table 1. Imaging sequence across the subjects. Each subject received a different set of images during the second cradle revolution. All rabbits received each imaging set in the table, except for imaging revolution 2 where the set varied between animals as described. 0° refers to the cradle in its normal position.
| Imaging sets | #Scans | Cradle rotation increments |
|---|---|---|
| Slow CBCT | 1 | 0° |
| CBCT revolution 1 | 8 | 0°–315°, in 45° increments |
| CBCT revolution 2 |
8 | 0°–315°, in 45° increments |
| Fluoroscopy (fixed gantry, rotating subject) | 2 | Continuously rotating |
aRabbit 1 underwent this series of images twice. bRabbit 2 scanned with slow CBCT pre-set for this series. cRabbit 3 scanned at 15° offset increments for this series.
Table 2. Image acquisition settings.
| Scan type | kV | mAs | Projections/s | Acquisition time (s) | Angle range (°) | Rotation speed (°/s) |
|---|---|---|---|---|---|---|
| Standard CBCT | 100 | 148 | 15 | 33 | 200 | 6 |
| Slow CBCT | 100 | 594 | 15 | 132 | 200 | 1.5 |
| Fluoroscopy | 100 | 0.3 | 15 | 120 | 360 | 3 |
aOnly the cradle rotated for fluoroscopy mode, while only the x-ray imager rotated during the CBCT modes.
2.2. Registration analysis
All CBCT were reconstructed on the TrueBeam system and imported to VelocityAI 3.2 (Varian Medical Systems, Palo Alto CA) for analysis. For each image, the fixed-increment rotation was registered back to the previous zero increment image. After each complete rotation (subject returns to zero), the image was registered back to the initial image for that rabbit, to assess reproducibility across subsequent revolutions.
For each CBCT, three image registrations were performed sequentially: (i) a manual rigid registration of the cradle was performed to remove the known applied cradle rotation offset from further registration results (e.g. to place all images in the same frame of reference). It was also used to determine the actual rotated position against the intended applied rotation on the cradle and hence the accuracy of the applied cradle rotation, and to verify concentricity of the rotation; (ii) A 6DoF rigid image registration (RIR) was performed using a mix of automatic and manual alignment to bony anatomy of the overall subject's thorax. This was a global registration, to account for movement within the external envelop formed by the immobilisation and not to account for any soft tissue differences. Where rigid alignment was difficult due to bony anatomy changing between two images (e.g. vertebral column flexion), priority in registration was given to vertebrae, ribs and chest wall, in that order; (iii) Deformable image registration (DIR) was performed using the rigid registration as a starting point. B-spline registration was run using the finest spline resolution available (5 mm), applied to a bounding box covering the whole thorax. The DIR was used to quantify all non-rigid body movement (between parts of the bony anatomy, and both within soft tissue organs and the external skin contour).
The rigid translation vectors were extracted for assessment of global translations, while the deformation vector field (DVF) was exported for the DIR. A histogram of the DVF was extracted for assessment of the localised deformation.
2.3. Respiratory motion
For each 4DCBCT at the zero-increment position, the respiratory motion was characterised by tracking the most superior position of the diaphragm in each phase-bin set, and a spline fit was generated. This was also performed for the 4DCBCT of rabbit 2 with cradle rotation.
3. Results
The rotation cradle was aligned to the linac imaging isocentre within <0.5 mm using a series of CBCT images at different rotation points, and the computer controlled fixed increments of rotation were verified to be accurate with a mean deviation of 0.2° based on image registration of the cradle itself. All rabbits were successfully imaged during the anaesthetic time frame, and all planned images were collected. Figure 3 shows example slices from each CBCT in a revolution series for one rabbit.

Figure 3. An example of the CBCT acquired at each cradle rotation offset for a full revolution of rabbit 1. Transverse plane views through thorax on top row and vertical plane views on bottom row.
Download figure:
Standard image High-resolution image3.1. Rigid component of gravity-induced motion
The mean 3D magnitude of rigid registrations of the subjects was 5.7 ± 2.7 mm across all rabbits and revolutions. The absolute mean and maximum of each component of the registration is shown in table 3. Figure 4 shows the rigid registrations for all images, mapped over cradle rotation offset angle and for each translation component. This figure also demonstrates the reproducibility of rigid motion between revolutions as well as between subjects. Note the second revolution for rabbit 3 deviated more than the others as it moved within the immobilisation.
Table 3. The mean (and maximum) components from all the fixed increment registrations (mean of absolute values). Roll is reported as the mean difference from the nominal fixed offset roll averaged across all images. Translations and rotations are in units of mm and degrees, respectively.
| Registration mean (maximum) | Rabbit 1 | Rabbit 2 | Rabbit 3 |
|---|---|---|---|
| 3D magnitude translation (mm) | 3.9 (7.2) | 4.6 (7.3) | 6.7 (11.3) |
| LR translation (mm) | 2.6 (7.0) | 2.8 (5.4) | 4.9 (9.6) |
| AP translation (mm) | 2.1 (5.4) | 2.8 (5.3) | 2.6 (6.7) |
| CC translation (mm) | 1.1 (2.1) | 0.9 (1.9) | 2.4 (5.3) |
| Pitch (°) | 1.9 (5.5) | 0.8 (2.5) | 2.1 (7.8) |
| Yaw (°) | 1.2 (5.8) | 1.0 (2.1) | 0.8 (3.3) |
| Roll (°) | 5.3 (9.0) | 3.9 (5.9) | 6.2 (14.3) |
| Deformation (mm) | 0.2 (0.4) | 0.2 (0.3) | 0.3 (0.5) |

Figure 4. The translation magnitude of the rigid registrations as a function of rotation angle. The main motion is translation in the axial planes, with minimal changes cranial-caudal. The mean magnitude of rigid registrations was 5.7 ± 2.7 mm across all rabbits and rotations. Subject rotation was shown to be reproducible over cradle multiple rotations (shown by multiple lines for each rabbit).
Download figure:
Standard image High-resolution imageThe translational motion was reproducible for multiple rotations, within 2.1 mm, 1.1 mm, and 2.8 mm difference for rabbit 1, 2, and 3, respectively. Rabbit 3 was imaged with the finer 15° cradle rotation increments, however the trend in rigid registration followed the coarser 45° increment, indicating this is sufficient resolution.
3.2. Deformation component of gravity-induced motion
Residual thorax deformations were smaller than initial translational motion (table 3). Vector direction was qualitatively verified to ensure the registration was physical and realistic. A normalised cumulative histogram of the DVF magnitude was then generated (see figure 5). The 50th and 95th percentile for each histogram was also extracted, where the 50th percentile indicates the median deformation and the 95th percentile is reported to indicate maximum deformations (avoiding spurious results in the DIR where surface elements were stretched to non-physical results).

Figure 5. Cumulative histograms of thorax DVF magnitude (top row). Residual deformation is obtained after removing the translational registration above. All rotated images for each rabbit are shown (85 plots total). The deformations observed were smaller than the translational motion. The 95th-percentile of each DVF displayed a small dependency on cradle rotation angle (bottom row).
Download figure:
Standard image High-resolution imageThe mean DVF magnitude for all 50th percentiles was 1.2 mm (standard deviation 0.4; range [0.5, 2.5]) and for 95th percentiles was 2.6 mm (standard deviation 0.7; range [1.0, 5.2]). Each rabbit exhibited a different trend in maximum deformation vectors with rotation—rabbit 1 exhibited the clearest trend, peaking near 225°, after inversion; rabbit 2 peaked near 90°, prior to inversion, with most movement being lateral; rabbit 3 had less of a clear trend due to large lateral movement not observed in the other rabbits (due to the subject being less secure in the cradle), and maximum deformation was seen near 315° as it returned back to the zero cradle offset position.
3.3. Comparison of gravity-induced motion to respiratory motion
In the non-rotated rabbit 4DCBCT, respiratory diaphragm motion of 2–5 mm was observed (figure 6). This was of a similar magnitude to the total mean 3D gravity-induced translations (5.7 ± 2.7 mm), and larger than the deformation vectors (mean and absolute maximum 0.2 ± 0.1 mm and 5.4 ± 2.0 mm respectively).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Figure 6. (a) Respiratory motion of the rabbits without rotation, as observed using diaphragm cranial-caudal motion. (b) Rabbit 2 4DCBCT diaphragm motion for each cradle rotation offset.
Download figure:
Standard image High-resolution image{kind=link}
Additional imaging of rabbit 2 for 4DCBCT acquired at fixed 45 increments showed the respiratory motion had amplitudes in the range 1.5–2 mm and did not exhibit a clear trend with subject rotation (figure 6(b)). The segmented lung volume and surface area with rotation angle on the 3D CBCT also did not have any clear trend with rotation, but did vary up to 8% and 15% respectively across the rotated offset scans.
4. Discussion
In this paper, we rotated three rabbits and measured the gravity-induced motion with CBCT. Our results indicate that gravity-induced motion is primarily translational rather than rotational or deformation in small animals. In terms of magnitude, the translational/sliding motion of the animals was approximately 80% of the observed motion, and was highly reproducible for two of the three subjects. The gravity-induced deformations were of lower magnitude than normal respiration. It is still to be seen how the motion would scale with size and weight in the range of a human.
While the gravity-induced translations were large, these can be mitigated with purpose-designed, well-executed immobilisation systems. This is especially important for future studies in larger animals. A suitable patient rotation system has been designed for the fixed gantry Nano-X Tatum prototype, featuring pressure-controlled airbags and straps in addition to standard radiotherapy fixation devices (Feain et al 2017a). An MRI-compatible patient rotation system has also been designed and investigated (Whelan et al 2017).
A source of uncertainty in the results presented is the resolution of the CBCT and DVF. The images used in this work were reconstructed with the standard clinical CBCT voxel cranio-caudal dimension of 2 mm. The cranial-caudal length of the rabbit lungs was 30–35 mm, which meant there was limited information in this dimension. However, the 4DCBCT images were reconstructed with isotropic 0.25 mm voxels to better quantify the small scale of diaphragm movement. Comparison of DIR with the higher and lower resolution reconstructions did not lead to significant changes in results.
The DIR algorithm used had a limitation of 5 mm spline grid resolution. This was large compared to the lung dimensions, however the deformed images had good visual agreement, indicating this limitation helped to regularise the DIR and maintain realistic solutions. After DIR, residual mismatch in deformably registered images was measured up to 2–3 mm in the thoracic region, and larger beyond (legs, spine flexion). This sets an inherent uncertainty to the DIR results, again indicating the role of immobilisation to fix the pose of subjects under rotation.
While it is difficult to generalise these results to larger subjects, small animal models provide a means of acquiring information that is not achievable with human subjects. It is a common limitation in radiotherapy that a human subject cannot be imaged at the frequency used in this study. A preliminary human experiment using a different imaging modality indicates deformations of a similar order of magnitude (Whelan et al 2017). In that study, for MR pelvic imaging of a study of a single volunteer human under a single rotation, the prostate, bladder and rectum showed a mean rigid displacement of structure surfaces by 3–6 mm, and mean organ surface deformation of 1–3 mm.
To date there are no other published studies to the authors knowledge that investigate internal anatomy deformations under gravity induced rotation with x-ray imaging. While prototype small animal irradiators envisaged fixed sources and rotation stages rotate about a vertical axis, which negates the impact of gravity induced motion (Matinfar et al 2009), the commercial units have horizontal subject stages and rotating x-ray gantries (PXi Precision X 2015, Xstrahl Medical 2015). Vertical CT (Shah et al 2009) and seated fixed-beam treatments (Pankuch 2015, McCarroll et al 2017) are under development. Many cancer patients would be unable to maintain an immobilised upright or seated stance such as this over the course of radiotherapy treatment, or it may be undesirable as it limits the available beam entry paths to treatment areas. As the scientific and technical challenges are addressed, a longitudinal rotation patient support system could provide a singular solution to a fixed gantry radiotherapy delivery system.
We are advancing these pre-clinical results to clinical applications through two separate studies. We have ethics approval to perform a 100-patient study of their experience in a novel radiotherapy patient rotation system described in Feain et al (2017a). We are in the process of obtaining ethics approval for a 30-patient study that, in addition to measuring the patient experience under rotation, will also acquire volumetric MRI imaging data. This imaging data will be used to quantify human anatomic deformation due to gravity and also the impact on treatment planning. The latter study will use the MRI-compatible patient rotation system described by Whelan et al (2017).
5. Conclusion
This novel study investigates gravity-induced motion from longitudinal rotation on live animal subjects. The results of this imaging study showed that deformations introduced by subject rotation were of the same magnitude as physiological motion from respiration. The proof-of-principle is shown in rabbits, with encouraging results showing promise for larger subjects. By collecting images at fixed rotation points, we collected a ground truth for further work to develop methods for CBCT reconstruction incorporating motion with fixed source and rotating subject.
The principle motion of the rotated subjects was translational due to movement of internal tissues inside the animal. The deformation of the anatomy under rotation was found to be equal in scale to normal physiological motion. This indicates imaging and treatment of rotated subjects with fixed-beam systems can use rigid registration as the primary mode of motion estimation. While the scaling of deformation from rabbits to humans is uncertain, these proof-of-principle results indicate promise for fixed-beam treatment systems, implying it may be possible to do image-guided radiotherapy with fixed-beam systems and achieve similar accuracy to that practiced in the current standard of care for lung cancer radiotherapy, i.e. image guidance based on respiratory-blurred CBCT scans.
Acknowledgments
The authors acknowledge the support of staff at Nelune Cancer Centre (Prince of Wales Hospital, Sydney) and Crown Princess Mary Cancer Centre (Westmead Hospital, Sydney) for this work. Partially funded by NHMRC Development Grant APP1118450.
Conflict of interest
Authors Feain and Keall are shareholders and directors of Nano-X Pty. Ltd, a radiation therapy machine which incorporates patient rotation. Authors Feain and Keall are inventors on several pending patents involving patient rotation during radiotherapy.