


Abstract
A serious fire developed in the core of a nuclear reactor at Windscale Works, Sellafield, northwest England, which led to the release of significant quantities of radioactive material into the environment during 10–11th October, 1957. In 1957, Windscale Works was operated by the United Kingdom Atomic Energy Authority (UKAEA), and on 15th October it was announced by the Chairman of the UKAEA that a Committee of Inquiry had been established under the chairmanship of Sir William Penney to conduct an investigation into the accident. The Committee sat at Windscale Works during 17–25th October, interviewed 37 people (some more than once), and examined 73 technical exhibits. The Committee reported to the Chairman of the UKAEA on 26th October. The Report of the Committee formed the technical basis of a UK Government White Paper (Cmnd. 302) published on 8th November, 1957, but the Penney Report itself was not published, and was only made public (at what is now The National Archives, TNA, Kew) in January, 1988. The original Report of the Committee of Inquiry is reproduced here from a copy of the Report supplied by TNA from TNA File AB 86/25.
Export citation and abstract BibTeX RIS

Original content from this work may be used under the terms of the Creative Commons Attribution 3.0 licence. Any further distribution of this work must maintain attribution to the author(s) and the title of the work, journal citation and DOI.
To the chairman, UKAEA
Chapter I introduction
- 1.You appointed the Committee of Enquiry on the 15th October with the following Terms of Reference: 'To investigate the causes of the accident at Windscale No. 1 Pile on 10th October, 1957, and the measures taken to deal with it and its consequences; and to report'.
- 2.The Committee sat at Windscale Works from 17th to 26th October inclusive, with a break of one day, during which time evidence was received from the Witnesses whose names are listed in Appendix A. The majority of these Witnesses were called by the Committee, but in addition an invitation was extended to any Windscale Works personnel to appear before the Committee if they had information to offer pertinent to the accident. Four such Witnesses came forward (Mr Evans, Dr Leslie, Mr Shackcloth and Mr Mowat). In addition, we received written evidence in the form of graphs, reports, minutes of meetings etc.* Some of these represented the results of calculations carried out during the Enquiry at the Committee's request.
- 3.We visited No. 1 Pile, the scene of the accident, and also No. 2 Pile, which was shut down in order that we could examine a Pile in shut-down conditions such as prevailed in No. 1 Pile before the accident. In addition, we visited the Health Physics Centre to inspect the records of monitoring surveys which had been carried out outside the Factory.
- 4.Our report is presented in the following sections:
| Chapter I | Introduction |
| Chapter II | Events leading up to the accident |
| Chapter III | Cause of the accident |
| Chapter IV | The measures taken to deal with the accident |
| Chapter V | The measures taken to protect the workers |
| Chapter VI | The measures taken to protect the public |
| Chapter VII | Conclusions |
| Chapter VIII | Recommendations |
Chapter II. Events leading up to the accident
- 5.The accident occurred in the course of a controlled release of stored Wigner energy from graphite.
- 6.The first time that Wigner energy was released in the Windscale piles occurred spontaneously in September, 1952. As a result of a study of this accident, a procedure was instituted for controlling releases of Wigner energy. Over the period to the end of 1956, eight such releases were carried out on No. 1 Pile. The general procedure has been to shut down the Pile, to arrange the appropriate instrumentation and then to cause the Pile to diverge with no coolant air flow, thus raising the graphite and uranium temperatures. By this means, the graphite is brought up to a temperature at which Wigner release is started. This has not always succeeded in annealing all the graphite in the Pile, e.g. in 1956 one attempt (in April) was completely unsuccessful and two others partially successful; that is to say, energy releases were recorded from certain regions of the Pile only, and pockets were left un-annealed.
- 7.Originally the procedure was to carry out Wigner releases after 20 000 cumulative megawatt days. Later this figure was increased to 30 000 megawatt days. The Windscale Works Technical Committee, in September 1957, considered a paper (reference IGR-TN/W.586) which recommended an increase to 50 000 cumulative megawatt days in view of the increasing difficulties of obtaining a successful release. Until more experience had been obtained, it was decided that the next release should be at 40 000 megawatt days. A Wigner release therefore became due in October, 1957.
- 8.A note on the loading of the pile is relevant at this stage. The Pile consists of a structure of graphite blocks pierced by horizontal channels on an 8¼'' square lattice pitch. Each channel contains a string of uranium fuel elements. For the purposes of charge and discharge the channels are arranged in groups of four, access to each group being by way of a charge hole in the front shield. In the middle of each of the groups is a channel of smaller diameter normally used for the irradiation of isotope cartridges.
- 9.At the material time, the Pile contained natural uranium and slightly enriched (1.28 Co) uranium in the fuel cartridges and a considerable variety of isotope cartridges.
- 10.There are vertical channels in the pile used for experiments connected with the civil reactor programme. At the time of the accident, all these channels were empty except one, which contained a small magnet under test.
- 11.On 7th October at 01.13 the Pile was shut down and the main blowers switched off in the preparation for the Wigner release. All necessary steps were taken to verify that the Pile was completely shut down. The thermocouples used for the following Wigner releases were then checked, and those which were unserviceable were replaced.*
- 12.The shut down fans were switched off and the door in the base of the chimney and the back inspection holes on the Pile roof were opened to minimise coolant air flow through the Pile. At 19.25 the Pile was made to diverge to generate nuclear heat for triggering off Wigner energy.
- 13.The procedure for Wigner release is to concentrate as much flux, and therefore as much heat as possible, in the front lower region of the Pile by suitable manipulation of the lower coarse control rods, the upper control rods having been disconnected when fully in.
- 14.At 19.25, the pile began to generate nuclear heat and the power level was gradually increased so that, by about 01.00 on 8th October, 1.8 MW was registering on the Pile power meter. (We have established that when the upper horizontal control rods are completely inserted, the ionisation chamber measuring pile power is masked. The power meter reads low. As, however, the Pile was being controlled on temperature recordings, the only effect was to alter the relation between the rod movements and the power changes and hence the 'feel' of the controls.)
- 15.It should be noted at this point that the operation of a Wigner release is the responsibility of the Pile Physicist and his two deputies, by virtue of their specialised knowledge. The Pile Control Engineers operate on the instructions of the Pile Physicists during Wigner releases. It appears that there is nothing in the nature of a Pile Operating Manual. The only written instruction which was produced for our inspection was a minute of 14th November, 1955, a copy of which is at appendix C. However, the Pile Manager informed us that there was a limit of 250 °C maximum cartridge temperature which, it had been laid down, should not be exceeded in the first instance during a Wigner release. This temperature was observed in two channels around midnight on 7th October; accordingly, control rods were run in again and the Pile was shut down by 04.00.
- 16.Most of the graphite temperatures rose in the manner normal in Wigner releases. However, according to the Physicist in charge and the Pile Manager, at about 09.00 on 8th October the general tendency was for the graphite temperatures to be dropping rather than riseing, and it seemed probable that unless more nuclear heat was applied, the release would stop.
- 17.We have carefully examined the thermocouple records on this point. They do not wholly bear out the observation reported in the previous paragraph. Undoubtedly, some of the graphite temperatures were falling and there were some in which no Wigner release was apparent; but a substantial number of the graphite thermocouple readings showed steady increases. We would not therefore endorse the observation that the general tendency was for the graphite temperatures to be dropping rather than riseing.
- 18.However, acting on the observation which he had made, the Physicist in charge decided to boost the release with more nuclear heating. (It should be noted that second nuclear heating had been utilised during three previous Wigner releases. On the first two occasions, in 1954 and 1955, it was not utilised until at least 24 hours after the last regional burst of temperature, and after all the graphite temperatures had been seen to be dropping. In 1956, all graphite thermocouples except one were showing a fall.)
- 19.The bottom rods were withdrawn and the Pile made divergent at 11.05 with the object of raising the maximum uranium temperature, which at that time was 300 °C to 350 °C. The uranium thermocouple readings show a sharp temperature increase when the Pile diverged for the second time. The highest uranium temperature recorded was in channel 25/27; the thermocouple reading for this channel rose by 80 °C to 380 °C in a matter of 15 minutes, with a maximum rate of rise of about 30 °C a minute. The thermocouple reading was reduced to 334 °C within 10 minutes by adjustment of the control rods. Nuclear heating was maintained at a lower level until 17.00, and during this period the highest uranium thermocouple readings rose to about 345 °C. At 17.00 the nuclear heating was terminated.
- 20.(It should be noted that the positions of the uranium thermocouples correspond to the readings of maximum temperature during normal operation, but that these are not the positions of maximum uranium temperature during a Wigner release (see also paragraph 42 below).)
- 21.During Wednesday, 9th October, the uranium temperatures as recorded show a maximum of 360 °C, while at 22.00 the highest value recorded was 340 °C. The graphite temperatures showed considerable variation, but the general tendency was for the temperatures to increase following the second nuclear heating. One graphite temperature in particular, in channel 20/53, which had shown a reading of about 255 °C at the time when the second nuclear heating was applied, continued to rise steadily, until by 22.00 it had reached a temperature of 405 °C.
- 22.The high temperature being recorded in channel 20/53 caused the Pile Physicist, at 21.00, to shut the chimney base and the inspection holes to allow the chimney draught to induce some flow of air from the Pile and thus cool it. The effects were not considered big enough and at 22.15 the fan dampers were opened to give a positive air flow through the reactor. The dampers were open for 15 minutes on this occasion. They were opened again for 10 minutes at 00.01 on 10th October, for 13 minutes at 02.15 and for 30 minutes at 05.10. This had a cooling effect on all graphite temperatures except 20/53, where the temperature rise was merely arrested.
- 23.The records from the pile stack activity meter show no special features during the early stages of the operation. There was an almost imperceptible increase in activity before and during the period of the first three damper openings. At 05.40, at the end of the fourth damper opening, there was a sharp increase of six curies. This was noted by the Physicist who was then on duty, but no special action was taken because he regarded it as the normal consequence of the first movement of air through the pile and up the stack. This increase was followed by a steady drop in the curve for about two and a half hours after which time stack activity rose steadily to a figure of 30 curies at 16.30 on 10th October.
- 24.The outlet duct air temperature remained stationary at about 40 °C until 07.00 on 9th October, but rose steadily thereafter. With peaks occasioned by the successive damper openings, it had reached 85 °C by 08.00 on 10th October.
- 25.The graphite temperature in channel 20/53 continued to rise after temporary reductions during the periods of damper opening, until at 12.00 on 10th October a temperature of 428 °C was recorded. The dampers were again opened for 15 minutes at 12.10 and for 5 minutes at 13.40. During these openings, the second and very large increase in stack activity, which has already been mentioned, was noted. At about the same time, a high activity reading on the Meteorological Station roof was reported.
- 26.These effects suggested to the operating staff the existence of one or more burst cartridges. At 13.45, the shut down fans were switched on as a preliminary move in an attempt either to use the scanning gear to detect any burst cartridges or alternatively to blow the Pile cool. At 14.30, the turbo-exhauster was switched on in order to scan for the burst slug. It was then found that the scanning gear was jammed and could not be moved. The Pile Manager informed us that at the end of previous Wigner releases the scanning gear could not be moved, presumably because of over-heating. On the present occasion it was immovable despite the fact that the Maintenance Section had worked on it the previous day (9th October) and had moved it.
- 27.Being unable to operate the scanning gear, recourse was had to the MX 119 to sample the air coming from the Pile for particulate activity. This showed a large positive reading.
- 28.At this stage, the Works General Manager was informed by the Pile Manager that there appeared to have been a bad burst, and he instructed that the affected channel should be identified and discharged as soon as possible.
- 29.Since the scanning gear could not be used, it was decided to remove the charge plug and inspect the uranium channel showing the highest readings.
- 30.Certain steps had to be taken before entry could be effected to the charge hoist. An air count had to be taken to ensure that there would be safe working conditions and the operatives themselves had to have a full change into protective clothing. When access had been secured to the charge hoist, a further delay of a few minutes ensued because of incorrect labelling of a thermocouple. The temperature of fuel channel 21/53 had been recording very rapid increases until at 16.30 it was in the neighbourhood of 450 °C. At this time, the plug covering this group of four channels was pulled out and the metal was seen to be glowing; the graphite appeared to have its normal colour. No sign of abnormality was observed in the isotope channels, but no positive conclusion can be drawn from this because the annular gap is much less in the isotope channels than in the uranium channels.
- 31.This is the appropriate point at which to end the present chapter, as it is clear from our enquiries that the accident had happened by this time; what followed were remedial measures, belonging appropriately to Chapter IV.
Chapter III. Cause of the accident
- 32.We have come to the conclusion that the primary cause of the accident was the second nuclear heating.
- 33.This was carried out between 11.05 and 17.00 on Tuesday, 8th October, when parts of the pile were still rising in temperature. Having regard to the high temperatures already existing in parts of the pile at this time, the second nuclear heating was too soon and too rapidly applied.
- 34.The rate of heating for a short period from 11.20 to 11.35 was particularly severe and caused a maximum rate of rise of the observed uranium temperatures of approximately 10 °C per minute.
- 35.The second nuclear heating led to the accident through a chain of events, and here we must put the possible consequences in order of probability. In our opinion, by far the most likely possibility is that the rapid rise of temperature of the fuel elements due to the second nuclear heating caused the failure of one or more of the fuel element cans. The exposed uranium oxidised and gave further release of heat, which, together with the rising temperatures occasioned by later Wigner releases, initiated the fire.
- 36.A second possibility, which we cannot entirely reject, is that a Lithium-Magnesium cartridge failed because the second nuclear heating triggered off pockets of Wigner energy at a time when the general level of temperatures through the pile was high. The oxidation of the Lithium-Magnesium could have added further heat and initiated the fire.
- 37.Once a cartridge had failed, whether it were Uranium or Lithium-Magnesium, the burning of the graphite would make some addition to the heat being released and would make its contribution to the development of the fire.
- 38.We have studied and rejected the possibility that the source of the fire was an isotope cartridge other than the Lithium-Magnesium type mentioned above. We have ascertained that the residual heating due to radioactive decay and gamma ray absorption is insignificant, and at most amounts to 3 °C.
- 39.We consider that the evidence points to the initiation of the fire being the result of the failure of the can of a fuel element giving rise to oxidation. We also consider that the origin lay in the region of the Pile just below the middle plane and towards the front.
- 40.The picture we have formed of this phase of the incident is as follows.
- 41.The uranium thermocouples were installed in all cases in cartridges about 16 feet from the front face of the Pile, where the maximum temperatures occur under normal operating conditions. Since 1954, these thermocouples have been used to control the progress of the nuclear heating for Wigner release.
- 42.The uranium thermocouple readings were lower than the maximum uranium temperatures elsewhere in the channels for two reasons. Firstly, the control rod positions were arranged to concentrate the nuclear heating in the front lower part of the Pile and we have examined a calculation which indicates that the peak neutron flux under these conditions was some 3 feet nearer the front face of the Pile than under normal operating conditions.
- 43.Secondly, every effort was made to minimise air flow through the channels to assist the nuclear heating in initiating the Wigner release; the position of the maximum uranium temperature thus corresponds to the position of peak neutron flux.
- 44.The combined effect of the distortion of neutron flux together with the transfer of the point of maximum temperature to coincide with the point of maximum flux resulted in the position of maximum uranium temperature occurring some seven feet nearer the front face of the Pile than the thermocouple positions. We estimate that the maximum temperature rise of the uranium could be 40% greater than the recorded temperature rise during nuclear heating.
- 45.The second nuclear heating was applied at 11.05 on 8th October, when the majority of the graphite temperatures and all the uranium temperatures in the channels in the affected region were rising, and when the maximum recorded uranium temperature in channel 25/57 was 300 °C. The rate at which nuclear heating was applied was unusually rapid and led to a recorded rate of uranium temperature rise of about 10 °C/minute to a maximum value of 380 °C at a point 16 feet from the Pile face. The normal practice in pile operation is to limit such rises to 2 °C/minute.
- 46.We calculated that at that point of peak neutron flux, where a graphite temperature in the vicinity was measured as 315 °C, the uranium temperature could initially have been at 340 °C. The maximum uranium temperature after the sudden nuclear heating could thus have been as much as 450 °C for some minutes.
- 47.That this treatment probably led to the immediate bursting of one or more uranium cartridges is deduced from the following.
- 48.Some of the Mark X fuel cartridges in the affected region had received an average of 287 MWD/tonne. Evidence was given to us that under normal operating conditions in the Windscale piles, bursts of this type of cartridge occur very infrequently at doses below 280 MWD/tonne, but that at higher dose rates bursts become increasingly frequent. With Mark X cartridges, the incidence of bursts has been mainly in the front end of the Pile, and many of these bursts have been caused by growth of the uranium rod causing a crack in the shoulder at the cartridge end.
- 49.We consider that in this way some cartridge bursts could have been produced during the early part of the second nuclear heating by the rapid differential growth of the uranium relative to the aluminium. The ends would have been pushed off cartridges which had already had a dosage which brought them into the state of increasing susceptibility to bursting.
- 50.Under these conditions, slow oxidation of the exposed uranium metal would occur. Laboratory tests have shown that complete oxidation of a uranium cartridge is possible within a period of 24 hours if the cartridge is held at a temperature of 400 °C inside a furnace. With sound undamaged cartridges the number of failures at this temperature would be extremely small, but with burst cartridges oxidation would be inevitable at 400 °C and would accelerate rapidly at higher temperatures.
- 51.It may be noted that the total heat of combustion of the uranium in a complete channel comprising 17 Mark X cartridges and 4 Mark VI cartridges amounts to the very large figure of 50 000 kilogram calories. Once the assumption is made that a single uranium cartridge is ignited, there is no difficulty in visualising several probable routes by which final conflagration can be reached. It is to be expected that slow combustion continued during the period of stagnant air conditions until 22.15 on 9th October, when the shut down air dampers were first opened to admit air to the pile.
- 52.The rate at which air will begin to circulate through a pile on first closing the chimney base and opening air dampers on the inlet side will inevitably be slow. This is due to the fact that the air in the pile will be stagnant, the chimney will be cold, and there will be little pressure difference available to draw air through the core. The first three periods during which the dampers were opened were too short to permit any steady current of air to be established through the pile. For this reason the fission product activity released from the oxidising fuel elements was not carried to the top of the stack. But on the fourth opening of the dampers (at 05.10 on Thursday, 10th October), lasting for 30 minutes, a sufficient flow of air was established through the pile to carry a cloud of gaseous fission products and also some particulate activity up to the filter at the top of the chimney. At 05.40, a sharp increase was recorded on the pile stack activity meter.
- 53.During this period, the intermittent supply of air to the pile caused an accelerated rate of oxidation of the smouldering uranium fuel elements in the affected zone. Slow combustion of uranium continued during the morning of Thursday, 10th October with locally rising graphite temperature. Switching on the shut-down fans at 13.45 had the effect of rapidly increasing the rate of combustion in the affected channels. By approximately 15.00, a serious fire was raging in the neighbourhood of the 20/53 group of channels.
- 54.The evidence which we obtained on the Lithium-Magnesium cartridges can be summarised as follows.
- 55.Of the various marks of can present, the most likely to have given trouble was the Mark III, which has a single can holding the alloy in the form of a rod. Laboratory tests have shown that above 427 °C, penetration of the can is possible as a result of the formation of a eutectic alloy. At 440 °C, all cartridges tested failed within 34 hours; at 450 °C, all failed in a few hours and some caught fire.
- 56.There is evidence from an analysis of particulate matter caught before 15.30 on October 10th by a cyclone filter at the top of the stack that some lithium and magnesium had burnt by then. However, no temperature as high as 400 °C was recorded in the graphite structure until 17.00 on Wednesday, 9th, and then only momentarily and in one graphite channel (21/48). For this reason, we consider it unlikely that the lithium-magnesium cartridges were the immediate cause of the fire.
- 57.For a portion of a graphite block to have been ignited at an early stage would also have required temperatures of 450 °C. The possibility of a local large release of Wigner energy in a pocket of graphite which had escaped previous annealing has been considered by us in the light of both thermocouple readings, laboratory data and general information. The available data indicate that the oxidation rate of graphite is very slow indeed at temperatures below 400 °C, and since we can find no evidence for the likelihood of serious 'pocket' releases or of temperatures in excess of 400 °C, we do not accept this as an explanation of the accident.
Chapter IV. The measures taken to deal with the accident
- 58.Immediately glowing metal was seen in the 21/53 group of channels, an attempt was made to discharge the fuel cartridges, but they were stuck fast and could not be moved.
- 59.It was considered inadvisable to switch on the main blowers in an endeavour to reduce temperature; in view of the high stack activity, this would probably have caused a serious neighbourhood hazard. The shut down fans had to be kept on, however, in order to maintain tolerable working conditions on the charge hoist. The workshops were requested, therefore, to make graphite plugs in order to blank off the over-heated channels. However, it was shortly afterwards found that in addition to the 21/53 group of channels detected by thermocouple reading, there was a rectangular region of some 40 groups of channels—about 150 channels in all—showing red heat. The attempt to make graphite plugs was abandoned, as it was now clear that the very large number required could not have been made in time.
- 60.From this time—at about 17.00 on 10th October—two principal remedies were attempted. Efforts continued throughout the night to discharge channels from the hot region. Early in the morning of 11th October it was necessary to bring scaffolding poles from the Calder construction site as the supply of steel push rods was giving out. Some of the hot channels were discharged by this means.
- 61.Secondly, at about 17.00 on 10th October it was decided to make a fire break by discharging a complete ring of channels around the hot region. This was successfully carried out. Later, a second row of channels was discharged above and at each side of the hot area; and later still, as the fire continued to threaten to spread upwards, a third row was discharged above the hot area. Discharge had to be suspended at one point while skips were moved, in order to avoid a criticality hazard in the water duct.
- 62.Two subsidiary measures were attempted with no success. The use of argon was considered, but it was found that insufficient quantities were available in the works. Secondly, a tanker of CO2 was brought over from Calder Hall, and arrangements were made for CO2 to be supplied to the hot channels. CO2 was fed into channel 20/56 at 04.30 but with no appreciable effect.
- 63.Meanwhile, observation from the top of the pile through the east inner inspection hole, revealed an obvious glow on the pile rear face at 18.45; at 19.30 the flames were much brighter, at 20.00 they were yellow and at 20.30 they were blue.
- 64.At about this time the use of water was first considered. Two hazards had to be examined: first the danger of a hydrogen-oxygen explosion which would blow out the filters, second a possible criticality hazard due to the replacement of air by water. The Management were informed, however, of the danger of releasing high temperature Wigner energy if the graphite temperatures were to rise much higher than 1200 °C. It was thought that this might well ignite the whole pile.
- 65.By about midnight the Works General Manager had decided that if the other measures failed to secure a reduction in temperature, water should be used. This was the major decision and it was supported by the Director of Production and the Deputy Works General Manager. The fire brigade was ordered to stand by with all available pumps, and work started on the preparation of equipment to enable water to be injected into the channels which had been discharged.
- 66.Shortly after midnight, the Chief Constable was warned of the possibility of an emergency and men in the factory were warned of an emergency with instructions to stay indoors and wear face masks.
- 67.At 01.38 the graphite in channel 20/53, near the top of the 'hot' area, showed a temperature of 1000 °C, and a fuel element temperature of 1300 °C was recorded by optical pyrometer. Over the next two hours, 'brute force' efforts were successful in discharging nearly all the top row of burning elements, but the fire continued unabated elsewhere.
- 68.By 03.44, the water hoses were ready to be coupled at 15 minutes notice.
- 69.Visual inspection at 04.00 through two of the pile roof inspection holes still showed blue flames: the graphite appeared to be burning.
- 70.After the unsuccessful use of CO2, temperatures continued to rise. Efforts to discharge the burning cartridges continued, but by 07.00 it was clear that the fire was not being checked. At 07.00, it was decided that water should be used, but that before it was turned on all factory labour should be under cover. Some delay was therefore necessary while the shift changed over at 08.00. Water was finally turned on at 08.55 and poured through two channels above the maximum height of the fire. From an initial rate of 300 gallons/minute the flow was increased to 800 gallons/minute. No dramatic change resulted; at 09.56 flames were still feathering out of the back of the pile. At 10.10, therefore, the shut-down fans were closed off to reduce air flow through the pile. The fire immediately began to subside. At 12.00, two more hoses were installed, and the water flow was increased to 1000 gallons/minute. The flow continued at this rate until 06.45 on 12th October, and was then gradually reduced until at 15.10 it had completely stopped. By this time the pile was cold.
Chapter V. The measures taken to protect the workers
- 71.On 10th October, between 11.00 and 14.00, a 3 hour air sample was taken outside the Health Physics Administration building. The sample gave a count of 3000 β dpm/m3 compared with a normal level of 200 to 300 β dpm/m3. This was one of the pieces of evidence indicating the probability of a burst cartridge, and this information was passed to the Assistant Works Manager and to the Pile Manager at about 14.00. From 14.15, half-hourly air sampling was undertaken over the Factory site, at some 10 to 15 different points.
- 72.Rising air counts led to an instruction, at 01.33 on 11th October, that workers should stay indoors and should wear face masks. At 02.30, when the activity appeared to be somewhat reduced, workers were instructed to remove face masks and to hold them ready.
- 73.The air contamination rose to a worrying but not dangerous level during the morning of 11th October. The values were patchy and varied with time. Expressed in terms of a maximum permissible exposure to any fission product in the air, by ICRP standards, for lifetime breathing, the values recorded rose from about two at 14.00 on 10th October to values in the region of five to ten during the night, with a few exceptional peaks as high as 150 on the following morning. By 12.00 on 11th October, the air activity was dropping fast and the value was one to two. The value of 2 was never again exceeded and most of the readings were about ¼ or less.
- 74.The highest readings on the morning of 11th October were around the chemical plants and the Calder site. There was no contamination, however, inside the buildings. The chemical plants were shut down and the workers instructed to sit in the main canteen; construction work on Calder B was stopped and the workers sent home. Earlier, workers had been instructed to stay within buildings at the time when the water was turned on.
- 75.When operations started on the No. 1 Pile charge hoist, standard procedure for health control was instituted. Special clothing and film badges were provided at a control point, and operatives were not allowed on to the charge hoist without full protective clothing and personal dosimeters. Special arrangements were made to ensure the rapid monitoring of the operatives involved. In the evening, extra staff were called in to man the surgery to deal with any severe cases of exposure, but there were none.
- 76.We have examined the total body radiation records of all the workers concerned in the accident. It is necessary to distinguish between exposure during the accident itself and exposure over the standard control period. The ICRP tolerance level, which was formerly 3.9 R per 13 week period, has recently been reduced to 3.0 R, and this is the standard now in force at Windscale Works. Over the 13 week period up to the 24th October, 1957 (i.e. including the accident), only 14 of the workers concerned in the accident exceeded the maximum permissible level. The highest figure recorded was 4.66 R. Records of exposure during the accident itself are not as reliable as the 13 week records, as the latter are taken from film badges, the former from quartz fibre electrometers, which give an approximate reading only. According to the QFE readings, two workers received 4.5 R during the accident, one 3.3 R, and there were four others in excess of 2 R. All the workers who received doses in excess of the maximum permissible level have been taken out of contact with work involving radiation, in accordance with standard procedure.
- 77.No worker had to be detained after the accident. Some had hair and hand contamination which was successfully removed by the standard decontamination procedure. One worker was not completely decontaminated at the first attempt, and his hands were gloved and his hair covered until the following morning when decontamination was successfully completed.
- 78.A thyroid iodine survey was made among the workers and is continuing. The ICRP level for safe continuous and constant iodine activity in the adult gland is 0.1 μc. The highest thyroid iodine activity so far measured among the staff is 0.5 μc. Since iodine has a short life, some increase over the ICRP level can properly be made if the dose occurs on a single occasion.
- 79.A survey is also being made among the workers for strontium activity, both Sr89 and Sr90. The radiochemical analysis takes time, and so far the two isotopes of strontium have not been measured separately. However, by making a reasonable partition of the activity marked between these two isotopes, the first 25 results which have so far been obtained show levels are at most one-tenth of the maximum permissible body burden.
- 80.The evidence so far on radioactive caesium is also satisfactory.
- 81.When the plugs were being removed from the charge wall to find the limits of the area of the fire and to eject burning cartridges, some men looked for a few seconds through the open plug holes towards the pile face from a distance of several feet back from the charge wall. A few men were not wearing head film badges, although they were wearing the normal type of film badge. These men might have had a dose to their heads, somewhere between 0.1 r and 0.5 r, in addition to the whole body dose recorded by their film badges.
- 82.During the morning of 11th October, the Windscale and Calder canteen managers consulted the Medical Department about their food supplies. They were instructed to take a few simple precautions and this they did.
Chapter VI. The measures taken to protect the public
- 83.A note of wind directions is necessary to appreciate some of the developments concerning public health. Throughout Thursday, 10th October, the ground wind was light, but mainly off-shore, i.e. NE or NNE. During the night it changed to NNW, and throughout Friday a 10 knot wind blew, mainly NW and NNW, i.e. down the coast. Still later it appears to have changed to a SW direction.
- 84.There may well have been an inversion at a few hundred feet above ground level during part of the period when radioactivity was escaping through the filter, and the winds above the inversion may not have been in the same direction as the ground wind. The fall-out pattern as it is now known strongly suggests meteorological conditions of this type.
- 85.At about 15.00 on Thursday 10th October, a survey van was sent out to make district surveys in the down-wind direction of the ground winds, i.e. along the cinder track towards Seascale. Because it is so much quicker to make gamma measurements than measurements of air activity, most of the measurements made were of gamma activity in order to cover the greatest possible area. The highest gamma reading recorded was 4 milli-r per hour on the Bailey Bridge near Sellafield station. This reading was mainly due to the activity in the plume. A second van was sent out at about 17.00 to the north of the factory, and likewise spent most of its efforts in measuring gamma activity in order to delimit the contaminated area. These two vans maintained continuous patrols throughout the night and the next day.
- 86.Some measurements, however, were made of the air activity on 10th October. The highest reading obtained was on the Calder Farm road at 23.00, and the value was about the same as in the Calder Works, i.e. some 10 times greater than ICRP level for continuous lifetime breathing.
- 87.The Health Physics Manager had to think of three kinds of hazard—gamma radiation to the whole body, inhalation and ingestion. In our opinion, he correctly decided that irradiation and inhalation were likely to prove well within acceptable limits for the district, and that the main concern should be ingestion.
- 88.For a time, the Health Physics Manager thought that the activity which was escaping from the top of the stack was normal fission products, and he therefore had to plan on the assumption that the main risks would come from iodine and strontium. By Friday morning, he had obtained the first analysis of the milk samples and the first results on the activity collected from the air in the Windscale Works. There was agreement that the activity contained a far greater proportion of iodine activity than would normal fission products. Having obtained this result, the explanation was clear: iodine vapour had come through the filter, but the major part of the particular material had been caught by the filter.
- 89.The deposition of iodine 131 on grass which is eaten by cattle is quickly carried to their milk, and a major part of the effort of the teams assessing the activity in the district has been given to milk analysis for iodine.
- 90.No established tolerance level existed for radioactive iodine in milk but the Health Physics Manager had in mind paper ARC/RBC 5 by Dr Scott-Russell, which suggested 0.39 μc per litre as the level beyond which iodine in milk would be a hazard to infants.
- 91.The first analysis of milk showed iodine 131 contents ranging from traces to 0.48 μc per litre, but when the analysis of the Seascale morning milk of Saturday, 12th October was completed at 15.00 and showed 0.8 μc per litre, the Health Physics Manager advised the Works General Manager that in his opinion the distribution of the milk gathered from the immediate vicinity of the Works should be stopped.
- 92.There followed several hours of consultation by telephone and by meetings between the medical and health physics experts, in order to establish the limit of radio-iodine content beyond which milk should be taken out of distribution. This was calculated, by reference to probable absorption into the thyroid glands of young children, at 0.1 μc per litre, a figure which was subsequently endorsed both by the Authority's medical consultants and by a meeting specially convened by the Medical Research Council as representing a reasonable assumption.
- 93.This decision was reached at about 21.00 on 12th October, and by arrangements made locally with the Cumberland police and the Milk Marketing Board, milk deliveries from 12 milk producers within a two mile radius of Windscale were prevented that night. Throughout Sunday and Monday, milk samples were collected from farms at increasing distances from Windscale. The scientific analysis was shared between the laboratories at Windscale and at Harwell. As the analyses were completed, the restriction on distribution had to be extended in successive stages, until by Monday morning it covered a coastal strip approximately thirty miles long, ten miles broad at the southern end and six miles broad in the north. To the south, it included the Barrow Peninsula and the northern boundary was about six miles north of Windscale.
- 94.Samples were also taken around the Lancashire Coast, the North Wales Coast, the Isle of Man, and into Yorkshire and the South of Scotland, but there was no necessity to extend the boundaries of restriction.
- 95.At the time of writing this report, the recorded levels are decreasing throughout the restricted areas; but no part of the area is yet sufficiently clear to enable the Authority to recommend to the Ministry of Agriculture, Fisheries and Food relaxation of the restriction.
- 96.Other possible sources of ingestion hazard were examined, in particular vegetables, eggs, meat and water supplies. None of these was found to be harmful.
- 97.A thyroid iodine survey has been made and is continuing among the local inhabitants around the works. The situation is similar to that among the people at the works. The highest thyroid activity measured among adults and children is 0.28 μc in the gland of a child. This level can be compared with the ICRP safe continuous level for adults of 0.1 μc in the gland. The results of the measurements made are under study by the Medical Research Council.
- 98.Parallel with the measurements of iodine activity are similar measurements on the two strontium isotopes Sr89 and Sr90. Enough results have now been obtained to suggest that there is no strontium hazard arising from the accident. Equally, there is no hazard arising from radioactive caesium.
- 99.It was represented to us that warning of an emergency ought to have been conveyed to the inhabitants of the area surrounding the Works. Two witnesses reported that high levels of activity had been measured on grass and on clothing in Seascale, and on clothing of people cycling to work along the track from Seascale on the morning of 11th October. The Health Physics Manager was satisfied, from the district measurements already mentioned, that no district radiation or inhalation hazard existed: there was therefore no occasion to issue a district emergency warning, which would have caused unnecessary alarm. The activity measured on the clothing of the two witnesses mentioned above was some 20 times lower than that which would have constituted any hazard in accordance with the standards observed by the Authority and based on the Medical Research Council tolerance levels.
Chapter VII. Conclusions
- 100.Our conclusions on the three points specifically referred to us are as follows.
- (a)The cause of the accident was as described in chapter II.
- (b)The steps taken to deal with the accident, once it had been discovered, were prompt and efficient and displayed considerable devotion to duty on the part of all concerned.
- (c)The measures taken to deal with the consequences of the accident were also adequate. There has been no immediate damage to the health of any of the public or of the workers at Windscale, and it is most unlikely that any harmful effects will develop. No physical damage has been sustained to property other than to No. 1 Pile.
- 101.A major technical defect contributing to the accident was the inadequacy of instrumentation for the safe and proper operation of a Wigner release. The uranium thermocouples were correctly positioned for normal operations, but not for Wigner releases; moreover, in the condition of stagnant air which had necessarily been created within the pile, there was no means of detecting the smouldering uranium cartridges, which we believe to have been a key event in the development of the accident.
- 102.The absence of an operating manual for Wigner releases must be regarded as a serious defect. Brief instructions, such as the minute reproduced in appendix C, are clearly inadequate, particularly for the circumstances prevailing in a second nuclear heating. We were obliged to piece together the other details of pile operation from Committee minutes and from traditions which did not seem to have any written authority.
- 103.One minor point should be mentioned. The Pile is a very large structure, and during a Wigner release operation it is frequently necessary for the people in charge of the release to climb some 70 feet to the roof in order to inspect the thermocouple readings. There is no lift; its absence must have added considerably to the operational difficulties.
- 104.The evidence which we received revealed deficiencies and inadequacies of organisation.
- 105.The division of responsibility between the Operations Branch, the Research and Development Branch of the Industrial Group, other technical branches within the Industrial Group and technical advisers at Harwell is not, in our opinion, clearly defined. Technical changes made by one team within the Authority have not always been known to others who should have been aware of them for the proper discharge of their technical responsibilities, and in some cases have not been adequately taken into consideration by those who were aware of them. There is uncertainty as to who is responsible for particular technical decisions, and there is undue reliance on technical direction by committee.
- 106.The operations staff at Windscale are not well supported in all respects by technical advice. For example, it appears that the records of recent Wigner releases had not been discussed by the Windscale Works Technical Committee. It appears also that changes have been made in operating procedures, with a general tendency to push pile temperatures upwards, without complete realisation of all the technical factors involved. We feel that since the Windscale Piles were handed over to the operations staff, other demands on the Industrial Group have been so heavy that insufficient technical attention has been available to ensure the safe operation of the Windscale Piles.
- 107.In our view, one of the lessons of the accident is that the Windscale organisation is not strong enough to carry the heavy responsibilities at present laid upon it. The responsibilities of the Works General Manager include the Calder Hall and Chapelcross reactors as well as Windscale. No one individual should be expected to exercise day to day operational control of so vast an organisation. We understand, moreover, that several of the posts in the Windscale complement under the Works General Manager were unfilled at the time of the accident.
- 108.The evidence which we received indicated that, when the accident occurred, the several responsibilities of the Chief Safety Officer, the Group Medical Officer and the Windscale Health Physics Manager were not clearly defined. Moreover, it appears to us to be unsatisfactory that tolerance levels in respect of several of the possible hazards should have had to be worked out in haste after the accident happened.
- 109.While in the above conclusions we have naturally concentrated on the faults and deficiencies, we must pay tribute to the efficient and energetic way in which the accident was dealt with once it was appreciated. Due to the efforts of the Windscale staff, a worse accident was averted.
Chapter VIII. Recommendations
- 110.Conscious of the great public anxiety concerning this accident, we felt we should report as soon as we had been able to consider the technical evidence sufficiently to discharge our terms of reference. We have not, however, in ten days been able to make a full technical assessment of all aspects of this matter. Moreover we are not properly constituted to recommend detailed organisational changes.
- 111.We therefore recommend:
- (a)That a Technical Evaluation Working Party should be set up within the Authority to make an urgent and thorough study of all the technical information to be derived from the accident. The technical records and reports which have been made available to us are being preserved in order that they may be studied by such a group.
- (b)That the Authority should review the organisation of the Industrial Group with regard to the relationship between the operational staff of the Windscale Piles and other technical directorates, and the adequacy of staff both in numbers and quality to cope with the responsibilities laid upon them.
- (c)That the responsibilities within the Authority for control of health and safety should be clarified.
- (d)That steps should be taken to ensure that maximum permissible levels are laid down for all radioactive substances for exposure for a limited period as well as for continuous exposure. (We recognise that the responsibility for this does not rest solely with the Authority.)
- (e)That Pile No. 2 should not be restarted until its instrumentation is fully adequate for the safe operation of a Wigner release, and until a careful review has been made of the factors involved in the controlled release of Wigner energy.
26th October, 1957
Appendix A
Witnesses examined (in chronological order)
| Mr H G Davey | Works General Manager, Windscale |
| Mr R Gausden | Manager (Pile Group), Windscale |
| Mr T G Hughes | Assistant Works Manager, Windscale |
| Mr K B Ross | Director of Operations, Industrial Group |
| Mr T Tuohy | Deputy Works General Manager, Windscale |
| Mr J C Bell | Senior Scientific Officer (R & DB), Windscale |
| Dr H K Hardy | Deputy Head of Laboratories (R & DB), Springfields |
| Mr J Wright | Atomic Energy Research Establishment |
| Mr K Saddington | Deputy Head of Laboratories (R & DB), Windscale |
| Mr W B Hall | Senior Principal Scientific Officer (R & DB), Windscale |
| Mr J Simmons | Atomic Energy Research Establishment, Harwell |
| Mr P W Mummery | Atomic Energy Research Establishment, Harwell |
| Mr C A Rennie | Atomic Energy Research Establishment, Harwell |
| Mr G S Towler | Chief Production Controller, Industrial Group |
| Mr C J Turner | Deputy Director Chemical Plants, Industrial Group |
| Mr W S Eastwood | Atomic Energy Research Establishment, Harwell |
| Dr J C Charlton | Radio Chemical Centre, Amersham |
| Mr J Moore | Research Manager (R & DB), Windscale |
| Mr J L Phillips | Works Manager, Dounreay |
| Mr P Jenkinson | Chemist III (Pile), Windscale |
| Mr D M Toole | Technical Class Grade II (Pile), Windscale |
| Mr B Cutts | R & D, Risley |
| Mr H Howells | Manager (Health Physics & Safety), Windscale |
| Mr R R Farmer | Chief Safety Officer, Industrial Group |
| Dr A S McLean | Group Medical Officer, Industrial Group |
| Mr L Rotherham | Director of R & D, Industrial Group |
| Mr E Davies | Engineer II (Maintenance), Windscale |
| Dr T E Graham | Senior Medical Officer, Windscale |
| Dr F M Leslie | PSO (R & DB), Windscale |
| Mr W J Hamer | Pile Control Engineer, Windscale |
| Mr S N Butler | Pile Control Engineer, Windscale |
| Mr J Morgan | Pile Control Engineer, Windscale |
| Mr R I Robertson | Physicist, Pile Group, Windscale |
| Mr W R Shackcloth | Training and Safety Officer, R & D, Windscale |
| Mr J S Mowat | SSO, R & D, Windscale |
| Mr V R Goodwin | Shop Manager, Pile Group, Windscale |
| Dr D W Williams | Senior Scientific Officer (R & D), Windscale |
Note: a number of the witnesses were recalled for further examination.
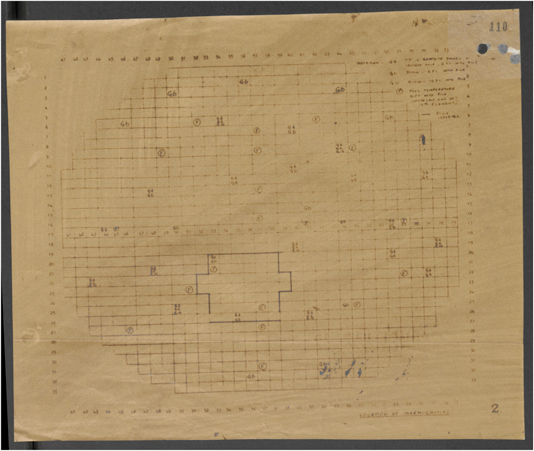
Appendix B.: Location of thermocouples
Appendix C
Mr Gausden
Wigner Energy Release
Will you please issue the following operating instructions to the operator engaged in controlling the Wigner energy release. If the highest Uranium or Graphite temperature reaches 360 °C, then Mr Fair, Mr Gausden and Mr Robertson are to be informed at once, and the PCE alerted, to be ready to insert plugs and close the chimney base. When the maximum temperature reaches 380 °C, unless further instructions to the contrary have been received, the roof plugs will be inserted and the chimney base closed. At 400 °C all of the dampers in the blower houses are to be opened and at 415 °C, 4 shut down fans are to be started up.
DRR Fair
Manager, Pile.
Copy to Mr Robertson
DRRF/RMcC November 14th, 1955
© Crown Copyright, 1957.
This information is licensed under the Open Government Licence v3.0. To view this licence, visit http://www.nationalarchives.gov.uk/doc/open-government-licence/ 
Footnotes
- *
Reproduction of the Report (the 'Penney Report') of the Committee of Inquiry (Chairman, Sir William Penney) established by the United Kingdom Atomic Energy Authority (UKAEA), which reported to the UKAEA on 26 October, 1957. The Report was made public in January, 1988, and the original can be found in The National Archives File AB 86/25.
- *
As this report was required urgently, it has not been possible within the time available to digest this material into properly edited appendices. Arrangements have, however, been made for its preservation (and see paragraph 111(a)).
- *
The location of the uranium and graphite thermocouples is shown at appendix B.