

Abstract
On 26 April 2016, thirty years will have elapsed since the occurrence of the Chernobyl accident, which has so far been the most severe in the history of the nuclear reactor industry. Numerous epidemiological studies were conducted to evaluate the possible health consequences of the accident. Since the credibility of the association between the radiation exposure and health outcome is highly dependent on the adequacy of the dosimetric quantities used in these studies, this paper makes an effort to overview the methods used to estimate individual doses and the associated uncertainties in the main analytical epidemiological studies (i.e. cohort or case-control) related to the Chernobyl accident. Based on the thorough analysis and comparison with other radiation studies, the authors conclude that individual doses for the Chernobyl analytical epidemiological studies have been calculated with a relatively high degree of reliability and well-characterized uncertainties, and that they compare favorably with many other non-Chernobyl studies. The major strengths of the Chernobyl studies are: (1) they are grounded on a large number of measurements, either performed on humans or made in the environment; and (2) extensive effort has been invested to evaluate the uncertainties associated with the dose estimates. Nevertheless, gaps in the methodology are identified and suggestions for the possible improvement of the current dose estimates are made.
Export citation and abstract BibTeX RIS
1. Introduction
The accident, which occurred at the Chernobyl nuclear power plant (NPP) in north-western Ukraine on 26 April 1986, resulted in widespread radioactive contamination in many countries of the northern hemisphere, particularly in Belarus, Ukraine and the Russian Federation. Following the accident, large amounts of radioactive materials were released to the atmosphere, including among those that are radiologically significant: short-lived iodine-131 (131I), tellurium-132 (132Te), iodine-133 (133I), and long-lived caesium-134 and caesium-137 (134Cs and 137Cs) (UNSCEAR 2011). The transport of these and other radionuclides caused substantial environmental contamination of the regions in Belarus, Ukraine, and the western part of Russia close to the Chernobyl NPP and resulted in enhanced exposure of the population (Bouville et al 2007). Two major groups of people were exposed to and, in some cases, are still being exposed to radioactive contamination: (1) members of the general public who resided or still reside in contaminated areas in Belarus, Ukraine and Russia, comprising those who were evacuated shortly after the Chernobyl accident; and (2) emergency and recovery operations workers (cleanup workers or liquidators) involved in the emergency response, containment, cleanup and other associated activities at the Chernobyl site and in the 30km zone around the NPP.
Following the Chernobyl accident, several analytical (e.g. Astakhova et al 1998, Stezhko et al 2004, Cardis et al 2005, Kopecky et al 2006, Tronko et al 2006, Worgul et al 2007, Romanenko et al 2008a, 2008b) and ecological (e.g. Jacob et al 1999, 2006, Likhtarov et al 2006, Pukkala et al 2006, Ivanov et al 2012) epidemiological studies were carried out or are currently in progress to quantify the risk of possible health consequences of the accident. These studies are focused on cancer, the main long-term effect expected in the population exposed to radiation, and on some non-cancer outcomes among the residents of the most contaminated regions in the three most affected countries as well as among the Chernobyl cleanup workers.
The main purpose of this paper is to critically review the methods used to reconstruct radiation doses in support of the Chernobyl epidemiological studies. We focus on the analytical studies (either cohort or case-control), for which individual doses have to be estimated for all study subjects. Well-designed analytical studies with reliable individual dosimetry provide a robust evaluation of exposure-related health risks compared to studies where dose information is only available at group or population level (dos Santos Silva 1999). Both environmental and occupational studies are considered. The paper also identifies gaps in the methodology and provides recommendations for improvement to properly support future epidemiological studies of the most informative exposed populations.
2. Estimation of doses and uncertainties in environmental studies
The general strategy to support dose estimation for analytical epidemiological studies among members of the public exposed to radiation after a nuclear reactor accident includes: (1) the identification of the target population, (2) the collection of as many individually-based radiation measurements as possible for subjects in the target population, (3) the collection of personal and lifestyle information that can be used for the estimation of an individual dose, (4) the collection of information on the spatial and temporal patterns and variations of the radiation field, (5) the calculation of realistic radiation doses with efforts to minimize sources of bias, (6) the validation of the dose estimates by independent measurements or strategies, and (7) the qualitative and quantitative evaluation of the uncertainties associated with dose estimates (Bouville et al 2014).
Based on this general strategy, the epidemiological studies of environmental radiation exposure have been classified into three categories:
- Category 1 includes studies in which dose estimates are based on individually-based radiation measurements available for all study subjects with provided and discussed uncertainties in dose estimates;
- Category 2 includes studies in which individually-based radiation measurements are not available for all study subjects and doses are therefore estimated by indirect methods based on extrapolation or modeling applied to all individuals, and the uncertainties in dose estimates are quantified;
- Category 3 includes studies in which individually-based radiation measurements are not available for all study subjects, so that doses are estimated by indirect methods, and the uncertainties in dose estimates are acknowledged but not quantified.
The majority of the Chernobyl-related analytic studies among members of the public are aiming to assess the radiation-related risk of thyroid cancer and other thyroid diseases. Therefore, the estimation of thyroid doses and their uncertainties is of major interest in this section of the paper. Thyroid doses after the Chernobyl accident arose essentially from the intake of 131I, a radionuclide with a physical half-life of 8.04 d that concentrates in the thyroid. For most individuals, 131I intake was due to the consumption of fresh cows' milk, cows' milk products and leafy vegetables; while the inhalation of contaminated air played a minor role. Other exposure pathways, including external irradiation from the gamma-emitting radionuclides deposited on the ground, the inhalation of short-lived radioiodines and radiotelluriums, and the ingestion of foodstuffs contaminated with long-lived radionuclides, were usually minor contributors to the thyroid dose (see, e.g. Gavrilin et al 2004).
The following information has been used to reconstruct individual radiation doses to the participants of the epidemiological studies carried out in Belarus, Ukraine and the Russian Federation:
- About 400 000 measurements of gamma radiation using detectors placed against the neck (called 'thyroid counts' or 'direct thyroid measurements') were made within a few weeks following the accident in the contaminated areas in Belarus, Russia, and Ukraine (Zvonova et al 1998, Gavrilin et al 1999, Likhtarov et al 2005). The results of the measurements were used to assess individual thyroid doses from the intake of 131I.
- The deposition density of 137Cs measured in essentially every settlement in the contaminated areas in Belarus, Russia, and Ukraine (EC 1998).
- The deposition densities of 131I and other radionuclides, such as zirconium-95 (95Zr), niobium-95 (95Nb), ruthenium-103, -106 (103Ru, 106Ru), 134Cs, cerium-141, -144 (141Ce, 144Ce), were measured in some contaminated settlements (Pitkevich et al 1996, Mück et al 2002, Drozdovitch et al 2013a, Khrushchinskii et al 2014).
- More than 500 000 whole-body counter (WBC) measurements of 134Cs and 137Cs body-burdens in residents of the contaminated areas were carried out during the post-accident years, starting in July 1986 (Likhtarev et al 1996, 2000, Minenko et al 2006);
- Measurements of monthly individual doses using thermoluminescence dosimeters (TLDs) distributed among residents of the most contaminated areas (see, e.g. Golikov et al 1999) were used mainly to confirm the validity of the dose estimation method;
- Measurements of thyroid volumes were carried out in the early 1990s by the Sasakawa Memorial Health Foundation in Belarus, Ukraine, and the Russian Federation (Ashizawa et al 1997).
2.1. Category 1: environmental studies
Only two cohort studies used individually-based radiation measurements available for all cohort members and provide evaluation of uncertainties in dose estimates. These cohort studies of individuals exposed as children and adolescents at the time of the Chernobyl accident were carried out in Belarus, by the Republican Research Center for Radiation Medicine and Human Ecology (Gomel), and in Ukraine, by the Institute of Endocrinology and Metabolism (Kyiv), in close collaboration with the U.S. National Cancer Institute (NCI, Bethesda) (Stezhko et al 2004). A unified study protocol and dose estimation approach was used in both studies, although there were differences in the techniques of the individually-based radiation measurements, and in the number and type of environmental radiation measurements.
2.1.1. Description of the cohort studies of thyroid cancer and other thyroid diseases in Belarus and Ukraine.
The two screening cohorts consist of 11 732 and 13 204 individuals in Belarus and Ukraine, respectively, selected from people who met the following criteria: (1) they resided in April–May 1986 in the most contaminated Gomel and Mogilev Oblasts and Minsk-city in Belarus; and in the northern part of one of the three most contaminated oblasts of Ukraine: Kyiv, Zhytomyr or Chernihiv (see figure 1); (2) their age was 0–18 y at the time of the Chernobyl accident; and (3) they were subjected to direct thyroid measurements performed between 26 April and 30 June 1986. These unique cohorts provide the basis for the estimates of radiation-related risk of thyroid cancer and other thyroid diseases in the exposed population (Tronko et al 2006, Brenner et al 2011, Zablotska et al 2011, Ostroumova et al 2013).
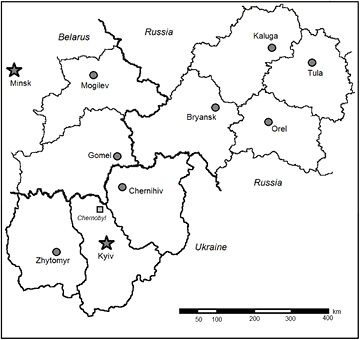
Figure 1. Oblasts of Belarus, Ukraine and Russia contaminated following the Chernobyl accident where the studies were conducted.
Download figure:
Standard image High-resolution imageEssentially, the same approach was used to calculate thyroid doses due to 131I intake for members of Belarusian and Ukrainian cohorts. The methodology is shown in figure 2 and is described in detail elsewhere (Likhtarov et al 2014, Drozdovitch et al 2015). In brief, information on residential history and dietary habits collected during personal interviews (box 1 in figure 2) was combined with data on 131I deposition densities at places of residence (box 2 in figure 2) and ecological and biokinetic models (boxes 3 and 4 in figure 2) to calculate the 'ecological' 131I activity in the thyroid, Aecol(k,T), at the time of the direct thyroid measurement, T (box 5 in figure 2) and the time integral of the 131I activity in the thyroid AIecol(k) (box 6 in figure 2). The 'ecological dose' Decol(k) (box 7 in figure 2) was then derived from AIecol(k) using the thyroid mass Mth(k) of the subject under consideration. The 'instrumental' 131I activity in the thyroid Ainst(k,T), which was derived from the individual direct thyroid measurement done at time T (box 9 in figure 2), was used to calibrate the 'ecological' 131I activity in the thyroid, Aecol(k,T), at the time of the direct thyroid measurement (box 5 in figure 2). The 'instrumental thyroid dose', Dinst(k), which is the dose assigned to each cohort member for epidemiological analysis (box 8 in figure 2), was obtained as the product of the ecological dose and of the 'scaling factor', SF(k), which is the term used to refer to the ratio of the instrumental and ecological 131I activities in the thyroid at the time of the direct thyroid measurement, Ainst(k,T)/Aecol(k,T), (box 10 in figure 2). In summary, the instrumental dose for subject k is calculated as follows:

where Dinst(k) and Decol(k) are values of instrumental and ecological thyroid-absorbed doses (mGy); K is a unit conversion coefficient equal to 13.82 (Bq kBq−1 g kg−1 J MeV−1 s d−1 mGy Gy−1); Eth is the energy absorbed in the thyroid per decay of 131I (MeV); Mth(k) is the thyroid mass of the subject under consideration (g); AIecol(k) is the ecological time-integrated 131I activity in the thyroid (kBq d); Ainst(k,T) and Aecol(k,T) are instrumental and ecological 131I activity in the thyroid, respectively, at the time of the direct thyroid measurement, T (kBq).
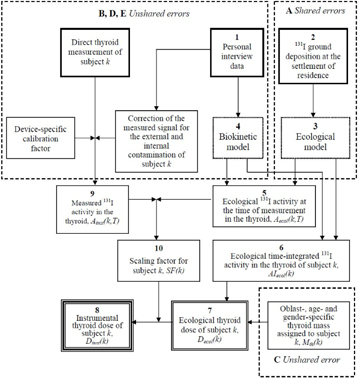
Figure 2. Scheme of thyroid dose calculation for the Belarusian cohort.
Download figure:
Standard image High-resolution imageThe four most important components of the thyroid dose estimation procedure are: (1) the direct thyroid measurements; (2) the measurements of 137Cs (and 131I) ground deposition densities; (3) the administration of personal interviews to all cohort members; and (4) the measurements of thyroid volumes among the populations of the contaminated areas.
2.1.1.1. Direct thyroid measurements.
The direct thyroid measurements, which are individually-based radiation measurements available for all cohort members, are the foundation used for the estimation of the instrumental thyroid doses. The quality of the direct thyroid measurements and, consequently, of the 131I activity estimates in the thyroids are better in Ukraine than in Belarus. The direct thyroid measurements were performed in Ukraine by professionals using spectrometric devices (about 40% of measurements) and SRP-68-01 survey meters that were collimated to reduce the radiation background. The uncertainties associated with 131I activity in the thyroid derived from direct thyroid measurements were well characterized and quantified (Likhtarev et al 1995). The results of the direct thyroid measurements performed with survey meters were corrected for internal contamination due to 134Cs, 136Cs, and 137Cs incorporated in the body (Likhtarov et al 2014).
In Belarus, the radiation-monitoring devices used for direct thyroid measurements, namely, DP-5 dose-rate meters, SRP-68-01 survey meters, and DRG3-02 dosimeters, were not designed to measure 131I activity in the human thyroid. Furthermore, measurements were performed not by professionals, but by people with no experience in radiation measurements. In general, the people who performed the measurements received instructions on how to use the measuring devices and to record the results of the measurements; however, there was no quality control of their measuring and recording practices. Quite often, the background exposure rate in the presence (or absence) of a subject in a room where measurements were performed, was not measured or recorded. To overcome these limitations, special efforts were made to evaluate the device-related uncertainties in direct thyroid measurements performed in Belarus (Khrutchinsky et al 2012) and to estimate the device response due only to the 131I content in the thyroid by elimination of the contributions to the overall signal registered by the device from other sources. The other sources were: (a) the background radiation in the room where the measurements were done, and (b) the external surface contamination of the body and the clothes as well as the internal contamination due to the presence of 134Cs, 136Cs, and 137Cs in the body.
2.1.1.2. Ground deposition densities of 137Cs and 131I.
The implementation of the ecological model that results in the calculation of the ecological thyroid doses is based on the daily ground deposition densities of 131I, which were often derived from measurements of 137Cs. Well-defined total 137Cs ground deposition densities have been measured in all contaminated areas of the territories of Belarus and Ukraine by their national Committees for Hydrometeorology. The daily deposition densities of 137Cs and 131I in Ukrainian settlements were calculated using the atmospheric transport model developed by Talerko (2005a, 2005b) for Ukraine. This model was adapted for Belarus using meteorological information, such as wind speed, wind direction, precipitation and temperature. The model calculations of daily 137Cs deposition densities were scaled to the daily measurements available for a few locations. In a second step, the model calculations of 131I deposition densities in Belarus were scaled to the 131I deposition densities measured in 508 Belarusian settlements (Khrushchinskii et al 2014).
2.1.1.3. Personal interviews.
Information on a person's whereabouts, the consumption of fresh cows' milk, cows' milk products and leafy vegetables, and the administration of stable iodine, which is required to estimate individual instrumental and ecological thyroid doses, was collected by means of personal interviews during two screening cycles. The study participants (or their mothers or close relatives, if a person was younger than ten years of age at the time of the accident) were interviewed at least twice in 1996–2007. The questionnaire used in the second interview cycle, both in Belarus and Ukraine, was improved by the Belarusian, Ukrainian and U.S. dosimetrists and epidemiologists following the experience gained from the first interview cycle.
Ideally, the behavior and dietary information collected for the study subjects should completely and precisely reflect what happened in the distant past. However, this is difficult to expect when the recalled period of interest and time of data collection are ten or more years apart (Byers et al 1987, Lee-Han et al 1989). The personal interview data for the majority of post-Chernobyl epidemiological studies were collected 10–20 and more years after the accident.
The majority of the cohort members or his /her relatives were interviewed at least twice between 1996 and 2007. The availability of repeated interviews made it possible to evaluate the reliability of the responses provided by the same study subject and their influence on uncertainty in the dose estimates, both ecological and instrumental (Drozdovitch et al 2016). It was found that, in general, the data collected during two interviews were rather consistent, answering general questions such as 'Did you move from your place of permanent residence?' or 'Did you consume milk?' As for more detailed information on dates and consumption rates, the agreement between the two interviews was inferior. The best recollection was found for residential history, milk consumption and, to a lesser degree, for stable iodine administration, while the consistency of the responses about the consumption of milk products and leafy vegetables was poorer.
2.1.1.4. Thyroid mass.
Thyroid mass is one of the most important parameters used in the estimation of the thyroid dose. Therefore, special studies were conducted to obtain thyroid-mass values that are the most adequate for children at the time of the Chernobyl accident. These age-dependent values were derived from ultrasound-based estimates of thyroid volume performed by the Sasakawa Memorial Health Foundation (SMHF) in 1991–1996 among about 57 500 Belarusian children (Skryabin et al 2010) and among about 60 000 Ukrainian children (Likhtarov et al 2013, 2014) who resided in the study areas at the time of the Chernobyl accident.
2.1.2. Estimation of the individual thyroid doses and of their uncertainties, accounting for shared and unshared errors.
The present state-of-the-art in dosimetry is to document the sources and quality of all input data, to establish a dosimetry error structure, to characterize each parameter used in dose calculations as a source of shared or unshared error, and to generate multiple sets of dose estimates for the entire study population. These multiple sets of cohort doses instead of a mean dose for each individual are being used to perform the dose-response analyses to estimate true risk (e.g. Li et al 2007, Stayner et al 2007, Little et al 2014, 2015, Land et al 2015, Stram et al 2015).
A Monte Carlo simulation procedure was used to estimate the uncertainties in instrumental thyroid doses received by the Belarusian (Drozdovitch et al 2015) and Ukrainian (Likhtarov et al 2014) cohort members. According to this procedure, 1000 sets of cohort instrumental thyroid doses, taking into account the classification of errors as shared or unshared, were calculated. This procedure is similar and generally consistent with the 2D Monte Carlo (2DMC) method (Simon et al 2015). For a specific dose realization, some of the model parameter values were common among the members of subgroups, i.e. shared among subjects of those groups, implying that any error made on this parameter was shared by all subjects to whom it applied. Subject-independent, or shared, parameters included parameters of the ecological model describing the temporal variation of 131I contamination in the ground, air, and foodstuff (box A in figure 2). Other uncertainties were considered to be subject-dependent, or unshared, including errors related to the 131I activity in the thyroid derived from the direct thyroid measurements (box B in figure 2), errors in assigning of thyroid-mass value to the study subject (box C in figure 2), biokinetic models of iodine in the human body (box D in figure 2), and the uncertainties attached to the imprecise answers on relocation history and individual diet from personal interviews (box E in figure 2).
Figure 3 shows the general scheme of calculation of 1000 sets of cohort doses taking into account shared and unshared errors. At the beginning of the calculation of each dose set for the entire cohort, values for all shared parameters were assigned. The same value for each shared parameter was used to calculate one dose set for all cohort members for whom this parameter was considered to be shared. This step introduced correlations in each cohort dose set between individual dose estimates of the study subjects who shared parameter values. In the process of dose-set simulation, the values of unshared parameters for each cohort member were sampled from their distributions and calculated, one dose realization for cohort member k, Di,k. The set of doses from Di,1 to Di,N represents a set number i of cohort thyroid doses for N cohort subjects. The thousand realizations of dose across the cohort dose sets for cohort member k, represent the individual stochastic thyroid doses of that cohort member.

Figure 3. Scheme of the calculation of multiple sets of cohort doses taking account of shared and unshared errors (adapted with permission from Drozdovitch et al (2015)).
Download figure:
Standard image High-resolution imageTable 1 shows the distribution of the arithmetic means of individual stochastic thyroid doses calculated for the Belarusian and Ukrainian study subjects. The global arithmetic mean of individual mean thyroid doses for the entire cohort was 0.68 Gy in Belarus and 0.65 Gy in Ukraine. The highest individual arithmetic mean of the individual stochastic doses among the study subjects was 39 Gy in Belarus and 42 Gy in Ukraine.
Table 1. Distribution (%) of thyroid doses from the intake of 131I among the subjects of the environmental studies of thyroid cancer in the general population.
| Thyroid doses (Gy) | Belarusian cohort |
Ukrainian cohort |
IARC-coordinated case-control study in Belarus and Russia (Drozdovitch et al 2010) | Belarus-NCI case-control study in Belarus (Gavrilin et al 2004) | Ukrainian in utero cohort (Likhtarov et al 2011) |
|---|---|---|---|---|---|
| <0.05 | 16.9 | 18.1 | 28.0 | 36.1 | 77.1 |
| 0.05–0.199 | 25.6 | 32.9 | 21.8 | 28.7 | 15.0 |
| 0.2–0.499 | 24.0 | 21.5 | 20.2 | 17.1 | 5.4 |
| 0.5–4.99 | 31.8 | 25.6 | 29.4 | 18.1 | 2.5 |
| 5–9.99 | 1.3 | 1.3 | 0.6 | — | — |
| ⩾10 | 0.4 | 0.6 | — | — | — |
| Arithmetic mean | 0.68 | 0.65 | 0.49 | 0.30 | 0.072 |
| Median | 0.27 | 0.19 | 0.20 | 0.11 | 0.012 |
| N of study subjects | 11 732 | 13 204 | 1615 | 321 | 2582 |
aDistribution is shown for the arithmetic mean of the individual stochastic doses.
The fitted distribution of the individual stochastic doses for each subject was found to be approximately lognormal and the geometric standard deviation (GSD) of that distribution was used to characterize the overall uncertainty for each individual. The GSDs varied from 1.3–5.1 with an arithmetic mean of 1.8 and a geometric mean of 1.7 over all subjects of the Belarusian cohort, and from 1.3–10.6 with an arithmetic mean of 1.6 and a geometric mean of 1.5 for the subjects of the Ukrainian cohort. In general, lower uncertainty in doses estimated in the Ukrainian cohort compared to the Belarusian cohort was mainly a result of higher quality estimates of 131I activity in the thyroid in the Ukrainian cohort and due to the uncertainty of the assigned dates of some thyroid activity measurements in Belarus. Table 2 shows the distribution of the GSDs attached to the individual stochastic thyroid doses for cohort members. The largest GSDs were associated with small 131I activity in the thyroid and were due to measurement uncertainties attached mainly to the calculated lower limit of the exposure rate in Belarus (Drozdovitch et al 2013b) and to measurement uncertainties associated with very small doses in Ukraine (Likhtarov et al 2014).
Table 2. Distribution of the GSDs attached to the individual stochastic thyroid doses from the intake of 131I in the Belarusian and Ukrainian cohorts.
| GSD interval | Belarusian cohort (Drozdovitch et al 2015) | Ukrainian cohort (Likhtarov et al 2014) | ||||
|---|---|---|---|---|---|---|
| N | % | Mean dose of the interval (Gy) | N | % | Mean dose of the interval (Gy) | |
| <1.5 | 4015 | 34.2 | 0.67 | 7982 | 60.5 | 0.66 |
| 1.5–1.99 | 6477 | 55.2 | 0.78 | 4711 | 35.7 | 0.68 |
| 2–2.99 | 1015 | 8.7 | 0.20 | 294 | 2.2 | 0.26 |
| ⩾3 | 225 | 1.9 | 0.29 | 217 | 1.6 | 0.017 |
The sensitivity analysis performed for the Belarusian cohort shows that sources of unshared errors associated with estimates of 131I activity in the thyroid and thyroid mass are the major contributors to overall uncertainty in the instrumental thyroid dose estimates. Shared errors associated with parameters of the ecological model were found to be small contributors to the overall uncertainty in the instrumental doses. Little contribution of shared errors was caused by the nature of the instrumental dose calculation. Indeed, to calculate the instrumental thyroid dose, the ecological dose was calibrated by the scaling factor that is the ratio of the measured to ecological131I activity in the thyroid at the time of measurement (see figure 2). Calibration of the ecological dose by the scaling factor eliminated the shared errors associated with the parameters of the ecological model, as the same values of shared parameters of the ecological model were used during the calculation of the given cohort dose set to estimate both the ecological dose and the ecological activity of 131I in the thyroid. However, the component of uncertainty in the cohort doses caused by shared errors was found to be significant for the ecological doses. The left panel of figure 4 shows the cumulative percentage distribution of 1000 ecological doses for the Belarusian cohort. Wide distribution indicates that the sources of shared errors are important contributors to the uncertainty of the ecological doses. In contrast, the shared uncertainties play a minor role in the overall uncertainty in the instrumental thyroid dose estimates (right panel of figure 4).
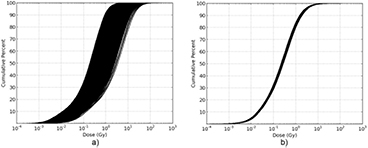
Figure 4. Cumulative percentage of 1000 cohort doses in Belarusian cohort: (a) ecological and (b) instrumental.
Download figure:
Standard image High-resolution image2.1.3. Validity of the thyroid dose estimates in Belarusian and Ukrainian cohorts.
As described above, to estimate realistic (instrumental) doses, the ecological dose was calibrated using a scaling factor that is the ratio of the instrumental to ecological 131I activities in the thyroid at the time of the direct thyroid measurement. The scaling factor is an indicator of the agreement between the dose estimated using the model and questionnaire data and the dose derived from direct thyroid measurement. The closer the scaling factor is to one, the closer the ecological dose is to the instrumental dose.
A wide inter-individual variability of the scaling factors was observed both in the Belarusian and Ukrainian cohorts. Neither the dates of the direct thyroid measurement and relocation, age of the study subjects at the time of the accident nor the occurrence of stable iodine administration were correlated with the scaling factors. The median values of the scaling factors were 0.81 in Ukraine and 0.35 in Belarus, thus indicating a bias in the results of either the direct thyroid measurements or the ecological model used in Belarus. Although the observed bias does not influence the estimated instrumental dose, this was eliminated in the Belarusian cohort by multiplying the scaling factors by 2.9. Figure 5 shows the distribution of the corrected scaling factors in the Belarusian cohort. The observed wide distribution can be partitioned into 3 categories:
- For about 86% of the study subjects, the corrected scaling factors were in the range from 0.1–10. This range was expected, given (1) the uncertainties related to the derivation of the 131I activity in the thyroid from the direct thyroid measurement, and (2) the uncertainties in the parameter values used in the ecological model.
- For about 13% of the study subjects, the corrected scaling factors were in the intermediate ranges (i.e. from 10–100 and from 0.01–0.1). Although the main reasons for these intermediate values are usually not clear, it is believed that they are due to a combination of factors, including biases in parameter values, complex residential histories, and difficulties in processing the direct thyroid measurements. In those cases, the uncertainties are somewhat underestimated.
- For about 1% of the study subjects, the corrected scaling factors were found to be very high (i.e. greater than 100) or very low (i.e. less than 0.01), and biases in the parameter values of the ecological model are not sufficient to explain these extreme values. An analysis conducted by Drozdovitch et al (2013b) showed that the possible reasons for obtaining the very low or the very large scaling factors appear to be: (a) imprecise and incorrect answers provided during personal interviews, (b) an assignment of direct thyroid measurement to a wrong subject, and/or (c) clerical errors in the recording of the direct thyroid measurement results. It is acknowledged that in those cases the uncertainty associated with the instrumental thyroid dose value may have been substantially underestimated. However, to assess the doses to all the study subjects in the same manner, it was assumed that the direct thyroid measurements were correctly performed and processed.
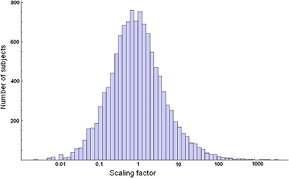
Figure 5. Distribution of the corrected scaling factors for the thyroid doses reconstructed for the Belarusian cohort members (adapted with permission from Drozdovitch et al (2013b)).
Download figure:
Standard image High-resolution imageAn evaluation of the importance of imprecise and incorrect answers provided during personal interviews was performed following analysis of the responses obtained during the first and the second personal interviews. These questionnaire responses were used to calculate two sets of ecological and two sets of instrumental thyroid doses due to 131I intake for each study subject. Figure 6 compares the individual ecological (left panel) and instrumental (right panel) thyroid doses calculated using information from the first and second interviews. As can be seen from figure 6(a), the ecological thyroid doses estimated for the same person using the results of different interviews were spread over five orders of magnitude. The ecological dose is directly proportional to the 131I deposition density in the settlement of residence, which together with the consumption pattern of contaminated foodstuffs determines the intake of 131I and, consequently, the ecological thyroid dose received by the study subject. Therefore, the low degree of agreement in the individual behavior and dietary data reported during two interviews led to the low degree of agreement between the ecological doses that were calculated using this information for each individual.
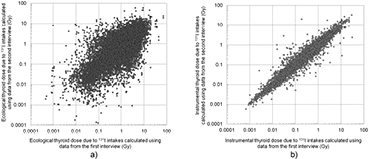
Figure 6. Comparison of (a) ecological and (b) instrumental thyroid doses due to 131I intake calculated using information from two interviews done among the subjects of the Belarusian cohort (adapted with permission from Drozdovitch et al (2016)).
Download figure:
Standard image High-resolution imageEssentially, better agreement was found for the instrumental doses (figure 6(b)), which were obtained by calibrating the ecological doses based on the result of direct thyroid measurement. The mean ratio of the instrumental dose calculated using data from the first interview to that calculated using data from the second interview for the entire cohort was 1.1 ± 0.7 while the median of the ratio was 1.0. It should be noted that although two sets of instrumental doses calculated using the two different interview data are, for the majority of compared doses, rather consistent, a substantial difference (<0.1 or >10 times) between the instrumental doses is observed for 23 out of 14 982 (0.15%) of the compared dose pairs (figure 6(b)). Further work is underway to understand the reasons for such discrepancies in the instrumental doses. However, it is important to conclude that, if the measurements are available for the study subjects, the quality of the individual behavioral and dietary data has, in general, a small influence on the quality of the retrospective exposure assessment (Drozdovitch et al 2016).
2.2. Category 2: environmental studies
Ideally, direct thyroid measurements are the most reliable form of information for dose assessment purposes, despite their associated uncertainties. However, not every individual residing in the contaminated regions of Belarus, Ukraine and Russia had direct thyroid measurement, including the subjects who were enrolled in the population-based case-control studies. For those lacking direct thyroid measurement, methods for dose reconstruction were developed and applied for all individuals included in the study. Two case-control studies of thyroid cancer are considered in this section.
2.2.1. IARC coordinated case-control study of thyroid cancer in young people of Belarus and Russia.
A population-based case-control study of thyroid cancer was carried out in the contaminated regions of Belarus (Gomel and Mogilev Oblasts) and Russia (Bryansk, Kaluga, Orel and Tula Oblasts) among people exposed to Chernobyl fallout in childhood and adolescence. The study included 1218 people from Belarus and 397 people from Russia who were 18 years old or younger at the time of the accident (Cardis et al 2005).
A working group, composed of dosimetrists and epidemiologists from Belarus, Russia, USA, France, Germany and Japan, was established to develop a unified approach to reconstruct individual thyroid doses due to 131I intake in the study subjects. The development of a common approach included four steps: (a) critical review of the four dosimetry models available for dose reconstruction in Belarus and Russia; (b) validation of the models by comparison of the modeled average age-specific thyroid doses for a settlement with average age-specific thyroid doses for a settlement derived from direct thyroid measurements; (c) validation of the two best performing models by comparison of the modeled individual thyroid doses accounting for the information obtained from personal interviews with individual thyroid doses derived from direct thyroid measurements; and (d) critical analysis of discrepancies observed in model predictions, and the selection of the best model for thyroid dose reconstruction (Drozdovitch et al 2010). The same steps were implemented for the models to calculate doses due to external irradiation and ingestion of Cs isotopes.
As a result of the validation study, a semi-empirical approach was selected to estimate the individual thyroid doses from 131I intake for the subjects of this case-control study. This approach was based on the relation between environmental contamination (137Cs or 131I deposition density) and the thyroid dose estimated from direct thyroid measurements carried out in population groups of various ages (infants, children, adolescents and adults) in the territories of Belarus and Russia with different contamination levels. Table 1 shows the distribution of the individual modeled thyroid doses due to 131I intake for the study subjects. The arithmetic mean of the individual thyroid doses for the entire study was 0.49 Gy. The highest individual dose due to 131I intake among the study subjects was 9.5 Gy (Drozdovitch et al 2010).
The validity of the modeled thyroid doses was confirmed by comparison with the instrumental doses. Fortunately, direct thyroid measurements were available for 63 study subjects from Belarus and 18 from Russia. A rather wide range of ratios between those two sets of individual doses was observed. The mean of the ratios of the modeled thyroid dose to the instrumental dose was 2.0 ± 2.2 and the median of the ratios was 1.2.
A Monte Carlo simulation procedure was used to calculate a set of 1,000 cohort (study population) thyroid doses from 131I intake accounting for shared and unshared errors in the dosimetry model (Drozdovitch et al 2007). In general, the approach used in this study was similar to that described in section 2.1.2. The GSD of the individual stochastic doses varied from 1.7–4.0 with median values of 2.3 and 2.1 for the Belarusian and Russian study subjects, respectively. The parameters of the semi-empirical model (shared errors) and thyroid dose per unit of 131I intake (unshared error) were identified to be the most important contributors to the overall uncertainty. The sources of shared errors were found to be relatively important contributors to the uncertainty of the modeled doses calculated in this study.
2.2.2. Case-control study of thyroid cancer in Bryansk Oblast in Russia.
A population-based case-control study including 66 cases of thyroid cancer (all aged less than 20 years old at the time of the accident) and 132 controls was carried out in Bryansk Oblast, which was the most contaminated region in Russia (Kopecky et al 2006). To reconstruct the thyroid doses due to 131I intake, a semi-empirical model was used. It was based on the relation between the environmental contamination (137Cs deposition density and the ratio of 131I-to-137Cs activity in deposition) and thyroid dose for adults derived from direct thyroid measurements carried out in 94 settlements in Belarus. The semi-empirical model was tested for application in Russia using thyroid dose estimates derived from direct thyroid measurements made in the Kaluga and Bryansk Oblasts (Stepanenko et al 2004).
Information about individual history of relocations, milk consumption and origin, and stable iodine administration was obtained during personal interviews of the study subjects, or their parents for subjects who were very young at the time of the accident. Dose adjustment factors were introduced to adjust the settlement average thyroid dose for adults to an individual dose, taking into account personal interview data.
The validity of the individual thyroid dose estimates in this study was confirmed by comparison with the instrumental doses for 19 people who were not study subjects, but resided in the study area and had reliable direct thyroid measurements. The mean ratio of the thyroid dose estimated using the semi-empirical model to that estimated using the direct thyroid measurement was 1.2 ± 0.99 and the GM of the ratio was 0.77; the distribution of the ratios was approximately lognormal with GSD = 2.9 (Stepanenko et al 2004).
The uncertainty in individual thyroid doses was estimated using a Monte Carlo calculation procedure. In this procedure, the values for all parameters used in the thyroid dose calculation were sampled repeatedly from their distributions (10 000 times each) to compute 10 000 estimates of the thyroid dose. In the implementation of stochastic dose calculations all sources of errors were treated as unshared. As in the IARC-coordinated study (section 2.2.1), the parameters of the semi-empirical model and thyroid dose per unit of 131I intake were found to be the most important contributors to overall uncertainty (Stepanenko et al 2004). The estimated GSDs of the thyroid doses varied among the study subjects from 1.8–3.5 and the median GSD was 2.2 (Kopecky et al 2006).
2.3. Category 3: environmental studies
Post-Chernobyl studies where uncertainties in dose estimates were acknowledged but not quantified (Category 3) include:
- A case-control study of thyroid cancer in Belarus, and
- A screening study of thyroid cancer and other thyroid diseases among Ukrainian individuals exposed in utero to 131I fallout.
2.3.1. Belarus-NCI case-control study of thyroid cancer in Belarus.
A population-based case-control study of thyroid cancer was carried out in the contaminated regions of Belarus by the Research Institute of Radiation Medicine (Minsk, Belarus) and NCI (USA). This study was the first analytical epidemiology study conducted on the population exposed after Chernobyl. A group of 107 cases, who were children at the time of the accident and who were diagnosed with thyroid cancer before 1 March 1992, and a group of 214 controls matched with the cases by sex and year of birth, and, to some extent, location, were included in the study (Astakhova et al 1998).
Children included in the case-control study were divided into three basic groups according to the type of radiation information that was available for the thyroid dose assessment (Gavrilin et al 2004):
- Children with direct thyroid measurements made in May–June 1986. The estimates of thyroid doses that were derived from these direct thyroid measurements were called 'measured' doses;
- Children without direct thyroid measurements, but living in those settlements where a reasonably large number of inhabitants had direct thyroid measurements. The age distribution of the average thyroid doses can be estimated for the children of those settlements with relatively good accuracy; the thyroid doses estimated using this method were called 'passport' doses; and
- Children without direct thyroid measurements and living in those settlements where such measurements were not carried out. To assess thyroid doses for these children, a dosimetric model based on the relationship between the measured 137Cs deposition or inferred 131I deposition and measured thyroid doses in comparable areas was developed (Gavrilin et al 1999). The thyroid doses obtained in this manner were called 'inferred' doses.
Table 1 shows the distribution of thyroid doses due to 131I intake reconstructed for the study subjects. The arithmetic mean of the individual thyroid doses for the entire study was 0.3 Gy. The highest individual dose due to 131I intake among the study subjects was 4.3 Gy. The uncertainties associated with the thyroid doses were not assessed analytically, but were assigned to each study subject depending on the group to which the subject belonged (Gavrilin et al 2004). For the group with 'measured' doses, the GSDs were estimated to vary from 1.7–2.6 depending on the quality of the direct thyroid measurement. For individuals with 'passport' doses, the GSDs ranged from 2.1–2.9 depending on the availability of information on individual milk consumption rates. The overall uncertainties attached to the estimates of the 'inferred' dose were characterized by GSDs of 2.2–2.8 if the milk consumption rate was relatively well known and 2.5–3.1 if the milk consumption rate was unknown.
2.3.2. Ukrainian in utero cohort.
A screening study of thyroid cancer and other thyroid diseases was conducted in a cohort of individuals exposed in utero to 131I fallout from the Chernobyl accident (Hatch et al 2009). The cohort comprised 2582 mother–child pairs in which the mother had been pregnant at the time of the Chernobyl accident on April 26, 1986 or in the following two months when 131I fallout was still present in the environment. Among these, 1494 were categorized as 'exposed'; a comparison group of 1 088 was considered 'relatively unexposed' (Likhtarov et al 2011). At the time of the accident, the women resided in some of the most contaminated territories of Ukraine: Chernihiv, Kyiv, Vinnitsa and the Zhytomyr Oblast.
To estimate the prenatal and postnatal thyroid doses due to 131I, the mother–child pairs were classified into three groups according to the availability of direct thyroid measurements:
- 720 exposed children with mothers who had direct thyroid measurement made in May–June 1986. Individual instrumental thyroid doses were calculated for these children;
- 774 exposed children whose mothers lived in contaminated settlements where thyroid activities were measured in other women, but not in their mothers; and
- 1088 children who belonged to a relatively unexposed group whose mothers resided in non-contaminated areas where direct thyroid measurements were not performed.
The estimation of the thyroid doses received by the subjects was based on (a) the results of the direct thyroid measurements performed on the mothers of the subjects or on women who lived in the same village as the mother of the subject; (b) responses on behavior and the consumption of milk, milk products and leafy vegetables provided during personal interviews of the mothers of the study subjects; (c) an ecological model of calculation of the 131I activity in the thyroid of the mother of the subject that takes into account the level of information available for that individual (Likhtarov et al 2005, 2006); and (d) a model of calculation of the in utero thyroid dose per unit intake of 131I by the mother (Berkovski 1999, ICRP 2001).
Table 1 shows the distribution of thyroid doses due to 131I intake reconstructed for this study. Individual in utero thyroid dose estimates were found to range from less than 1 mGy to 3.2 Gy, with an arithmetic mean of 0.072 Gy. The main sources of uncertainty in the dose estimates, which were identified but not quantified, are expected to be related to: (a) the transfer coefficient from 131I intake by the mother to the thyroid dose received by the child; (b) the determination of the gestational age at the time of the accident; and (c) the scaling factors for adjustment of the ecological dose in groups of children whose mothers did not have direct thyroid measurements (Likhtarov et al 2011).
2.4. Contribution of minor pathways to the thyroid dose
Thyroid doses for most of the subjects of the studies considered above were mainly defined by internal exposure from the intake of 131I. Other exposure pathways were usually minor contributors to the thyroid dose: (1) intake of short-lived radioiodines (mainly 132I and 133I) and radiotelluriums (mainly 132Te); (2) intake of long-lived radionuclides (mainly 134Cs and 137Cs); and (3) external irradiation from radionuclides deposited on the ground (mainly 140La and 95Zr in the short term and 137Cs in the long term). The methods used to assess the thyroid doses from the minor exposure pathways are described elsewhere (Likhtarev et al 2000, 2002, Likhtariov et al 1996, Pitkevich et al 1996, Golikov et al 2002, Balonov et al 2003, Gavrilin et al 2004, Minenko et al 2006).
The mean contribution of the minor pathways to the total thyroid dose was around 5% for the subjects of the studies conducted in Belarus, and about 10% for the subjects in Russia (Gavrilin et al 2004, Drozdovitch et al 2010, 2013b). Intake of 131I was by far the predominant pathway of thyroid exposure. However, the contribution of the minor pathways may be substantial for specific groups of individuals. For example, for the residents of Pripyat, a town located near the Chernobyl reactor site, who were evacuated about 36 h after the accident and relocated to a non-contaminated area, the contribution of short-lived radionuclides (132I, 133I, and 132Te) was estimated to be about 30% of the total thyroid dose (Balonov et al 2003). In another example, the individuals who resided in a non-contaminated area during the first two months following the accident, but then relocated to a contaminated area would have only been exposed to long-lived radionuclides, such as 137Cs.
3. Estimation of doses and its uncertainties in occupational studies among Chernobyl cleanup workers
Following the acute emergency phase of the Chernobyl accident, about 530 000 cleanup workers from the former Soviet Union were called from 1986–1990 to carry out cleanup activities on the reactor site and around the Chernobyl NPP (UNSCEAR 2011). The population of the Chernobyl cleanup workers was extremely heterogeneous and encompassed a broad variety of occupational groups: military, nuclear workers and specialists, construction workers, support staff. They were assigned by different ministries and organizations to perform different work (decontamination, repair and maintenance of NPP equipment, construction, scientific support and research, supply and logistics, etc.) at various locations (from roofs of the reactor building to remote locations at the edge of the restricted '30 km zone'). The cleanup workers were mainly exposed to doses from external irradiation that were monitored by means of personal dosimeters, group dosimetry (one personal dosimeter per group of cleanup workers), or group assessment (when the same value of 'individual' dose was assigned to all members of a group who performed the same task, based on a dose assessment carried out prior to the implementation of the task) (Chumak 2007). The results, called 'official doses', were recorded in the Chernobyl State Registries when they became available. In the state registries of Belarus, Ukraine, and Russia, official dose records (ODRs) are available for about 9%, 43% and 71% of registered cleanup workers, respectively (UNSCEAR 2011). In the Baltic countries, the ODRs were drawn from official documents confirming participation in the cleanup activities and are available for 82% of the members of the cohorts of Chernobyl cleanup workers in Estonia and Latvia, and for 69% in Lithuania (Kesminiene et al 1997, Rahu et al 2006). Although varying in quality and methods to obtain them, ODRs have been discussed and often criticized (e.g. Ilyin et al 1995, Chumak et al 2000, Bouville et al 2006, Chumak 2007, Kryuchkov et al 2012, Bouville and Kryuchkov 2014). It was shown that the ODRs are usually biased and tended to overestimate true exposure and, therefore, were considered not to be useful in analytical epidemiologic studies. Other dosimetry methods, particularly biodosimetry (stable and unstable chromosome aberrations, EPR), are only available for a limited number of cleanup workers with doses higher than the detection limit of these methods; they were essentially used to validate the modeled dose estimates (Chumak et al 2005).
Similar to the epidemiological environmental studies, studies of occupational radiation exposure among Chernobyl cleanup workers have been classified into three categories according to the endpoint:
- Category 1 includes leukemia studies in which (a) bone-marrow dose estimates from external irradiation are calculated using the RADRUE method based on personal interviews of all the study subjects, and (b) the uncertainties in dose estimates are provided and discussed;
- Category 2 includes thyroid-cancer studies in which (a) thyroid dose estimates from external irradiation are calculated using the RADRUE method based on personal interviews of all the study subjects, (b) thyroid dose estimates from internal irradiation are derived from the available direct thyroid measurements using the results of personal interviews of all the study subjects, and (c) the uncertainties in dose estimates are provided and discussed;
- Category 3 includes a cataract study in which (a) lens-of-the-eye dose estimates are based on ODRs that were corrected for known bias, and (b) the uncertainties in dose estimates are quantified.
3.1. Description and analysis of the RADRUE method
3.1.1. Description of the RADRUE method.
The RADRUE method (Realistic Analytical Dose Reconstruction with Uncertainty Estimation) was developed and extensively tested by an international group of experts (Kryuchkov et al 2009). The main ideology behind the RADRUE technique is very straightforward: it is based on the calculation of the external dose as a product of the exposure rate and irradiation time, with shielding taken into account. Mathematically, the external dose D (mGy) absorbed in the bone marrow (or another organ) during a cleanup worker's trip can be inferred from the summation of the products of exposure rate, duration, and shielding factor during each time interval when the person was exposed to radiation:

where Ci is the conversion coefficient from exposure to bone-marrow dose (mGy h−1 per mR h−1); P[x(ti),y(ti),ti] is the exposure rate (mR h−1) at the location [x(ti), y(ti)] and at time ti, where and when the cleanup worker was present; ▵ti is the time interval during which the cleanup worker performed a relatively brief but complete task; Li is the shielding factor for the working conditions (sometimes called the 'location factor'); and n is the number of (usually unequal) time intervals considered in the calculation. Any time that an individual spent working, commuting, sleeping, or resting within the 70 km zone was included in the analysis.
An important element of the RADRUE method is a questionnaire which includes detailed questions about (a) the cleanup workers' routes to and from their work place(s) in the 30 km zone, (b) details about the work they performed, and (c) the locations of the residence and rest quarters used during their stay at Chernobyl. In the case of deceased, or otherwise incapacitated subjects, two proxies were interviewed: (1) a next-of-kin (usually the spouse or a grown-up child), who provided information on the lifestyle, and occupational history, besides the work in Chernobyl and the health data of the subject, and also gave the names of colleagues, who may have worked together with the subject during his cleanup mission, and (2) one (or several, if work periods overlapped only partially) identified colleague(s), to retrieve information on the cleanup activities that were carried out by the subject. Obviously, there is a concern about the accuracy of the information on work history obtained during the personal interview as so many years have passed since the accident. It should be noted that all interviewers were trained and, more importantly, in particular in cohort studies of the Ukrainian cleanup workers, they were experienced cleanup workers themselves. Supporting material, such as booklets with maps, schemes and photographs of the facilities and buildings within the 30 km zone at various periods of the cleanup activities, a dictionary of jargon and terms used by the cleanup workers, as well as photographs of dosimeters were used to help interviewees to remember important elements of their work and rest while in Chernobyl. During the personal interviews interviewers also used special questions to stimulate memory recall of a respondent.
Another key element of the RADRUE technique was a proper interpretation ('reading') of each questionnaire performed by an extremely knowledgeable expert-dosimetrist. Special exercises were performed to check the repeatability of the doses estimated using the results of two interviews of the same subject, and to evaluate the effects of using questionnaire responses from proxies to estimate the doses to cleanup workers (Kryuchkov et al 2009).
Dosimetry experts, familiar with the organization and conditions of work in the 30 km zone, reviewed this information in detail and reconstructed each cleanup worker's type, location and duration of activities and itineraries. These itineraries were entered into the computer program for the RADRUE calculations and linked with the data from an extensive database on exposure-rate measurements and interpolated values to calculate the organ doses. In some cases, because cleanup workers may have overestimated the amount of time they spent in specific high-exposure-rate areas, results from the use of RADRUE were much higher than the permissible dose levels in force at the time of the work. Therefore, a dose constraint procedure was introduced in RADRUE, and the doses were estimated with and without constraints. Both doses without and with constraint were used for epidemiological analyses, although the latter were thought to be more realistic and were applied in the main analyses. A detailed description of the models used to estimate the doses due to external irradiation can be found elsewhere (Kryuchkov et al 2009).
3.1.2. Validity of doses estimated by RADRUE.
The validity testing involved various intercomparison exercises where RADRUE doses were compared by Kryuchkov et al (2009) to the most reliable dose estimates available for different groups of cleanup workers. These included 39 professional workers from the Ministry of Atomic Energy who wore calibrated personal thermoluminescence dosimeters (TLDs); 20 early responders (firemen, ChNPP workers from the reactor and turbine buildings, etc.) with dose estimates based on the quantitative analysis of unstable chromosome aberrations (dicentrics); and 68 other cleanup workers with dose estimates based on the measurement of electron paramagnetic resonance (EPR) in tooth enamel (table 3).
Table 3. Validity of RADRUE doses: results of intercomparison exercises (adapted with permission from Kryuchkov et al (2009)).
| Comparison of RADRUE doses with doses based on | Number of liquidators | Correlation between two sets of doses | Ratio of RADRUE doses to doses included in the comparison | |
|---|---|---|---|---|
| Mean ± SD |
GM |
|||
| TLD |
39 | 0.84 | 1.3 ± 0.6 | 1.2 |
| Unstable chromosome aberrations | 20 | 0.80 | 0.83 | — |
| EPR |
68 | 0.38 | 1.3 ± 1.2 | 0.80 |
aTLD: thermoluminescence dosimetry. bEPR: electron paramagnetic resonance. cSD: standard deviation; GM: geometric mean.
Figure 7 compares the doses calculated using the RADRUE method with the dose estimates based on personal TLD monitoring of the staff of the Administration of Construction No. 605 (AC-605) from the Ministry of Medium Machinery. The two sets of doses show reasonable agreement within the uncertainty range; the mean of the ratios of the RADRUE-estimated dose to TLD-based dose was 1.3, while the median of the ratios was 1.2. The RADRUE-estimated doses correlated well with the doses derived from analysis of unstable chromosome aberrations (r = 0.80): however, the mean of the ratios was 0.83 (table 3). This difference could be due to the fact that radiation exposure resulting from the passing cloud of radioactive materials released during the first day of the accident was not considered in the RADRUE doses calculated for early responders. Although only a moderate correlation (r = 0.38) between RADRUE-estimated doses and EPR-based doses was observed, the mean and the median of the ratios were close to 1.
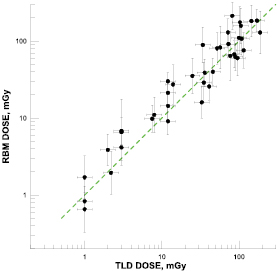
Figure 7. Comparison of the doses calculated using the RADRUE technique with dose estimates based on personal TLD monitoring of employees of the group AC-605. Error bars correspond to one GSD. The line indicates perfect agreement between the two sets of estimates (adapted from Kryuchkov et al 2009).
Download figure:
Standard image High-resolution image3.1.3. Uncertainties associated with doses estimated by RADRUE.
Two categories of uncertainties in the doses estimated by the RADRUE method were identified: 'intrinsic' and 'human factor' uncertainties (Chumak et al 2008). The first category includes uncertainties in exposure-rate data and soil-contamination measurements; uncertainties in the interpolation of these data in time and space; uncertainties in factors used to characterize the effectiveness of shielding; and imprecise answers from the questionnaire (e.g. failure to recall specifically the time of a particular cleanup mission). The second category includes uncertainties of recollection and reporting of the events related to the cleanup activities of a subject that occurred many years ago, especially when proxies were interviewed for deceased cleanup workers to estimate doses to cleanup workers. RADRUE takes into account only the 'intrinsic' component of uncertainty in the dose estimate, while 'human factor uncertainty' was not quantified (Kryuchkov et al 2009). Human factor uncertainty is being considered in depth in a separate study. Such a study, including the analysis of the work history reported by the cleanup workers shortly (weeks or months) after completion of their cleanup mission in 1986–1987, and of that obtained recently using the study questionnaire as well as the comparison of two sets of doses calculated using historical and recently reported work history, is currently underway.
In order to evaluate the intrinsic uncertainties, a Monte Carlo method was used to calculate 10 000 individual stochastic dose estimates for each study subject. No attempt was made to separate the shared and unshared errors in the calculations, but a sensitivity analysis was performed by Kryuchkov et al (2009) to evaluate the relative importance of the shared and unshared errors in the overall uncertainties of the RADRUE dose estimates. In brief, it was found that (1) the variability in the exposure rate contributed more than 96% to the overall uncertainty of the doses, while the variability of other parameters (location factor, frame duration, episode repetition, conversion coefficient) accounted for only a few percent of the overall uncertainty; and (2) the same location during the cleanup mission was shared by two cleanup workers at the same time in 0.13% instances and, as a result, the 'shared' dose represented less than 1% of the total dose among the study population. It is important to note that there are other sources of shared errors that have not been considered. For example, all the exposure rate measurements in the 4 km zone were made in 1986. Later, the exposure rates were extrapolated, and the uncertainties associated with that extrapolation were large. The doses to people working there after 1986 were all linked to the dataset used for the extrapolation. The same comment applies to the measurements made in other areas.
3.2. Category 1: occupational studies of leukemia and other hematological malignancies among Chernobyl cleanup workers
Two occupational studies are considered here:
- 1.The NCI- and University of Columbia-coordinated case-control study of leukemia in Ukrainian cleanup workers, and
- 2.The IARC-coordinated study of hematological malignancies in cleanup workers from the Baltic countries, Belarus and Russia.
3.2.1. Leukemia case-control study in Ukrainian cleanup workers.
In the framework of the Ukrainian–American collaborative project, a case-control study of leukemia and related disorders was conducted in a cohort of 110 645 male Ukrainian cleanup workers of the Chernobyl accident, who were exposed to various radiation doses over the 1986–1990 time period. The study included 1000 subjects and consisted of two phases. Phase 1 of the study included 572 subjects (Romanenko et al 2008a, 2008b), while phase 2 covered 428 subjects, for both cases and controls (Zablotska et al 2013). As already mentioned in section 3.1, all individual bone-marrow doses were calculated based on personal cleanup history data collected from an interview with the subject himself, if he was alive, or with two proxies, if he was deceased (Chumak et al 2008, 2015). The arithmetic means of the individual stochastic estimates of the bone-marrow dose range from 3.7 × 10−5 to 3260 mGy, with an arithmetic mean of 92 mGy for the entire study population (table 4). The GSDs (intrinsic uncertainty) of the individual stochastic external doses calculated by RADRUE varied among the study subjects from 1.2–5.9 with a mean equal to 2.0 (table 5).
Table 4. Doses (mGy) to the subjects of Ukrainian–American and IARC-coordinated studies of leukemia and thyroid cancer among Chernobyl cleanup workers.
| Pathway | Ukrainian–American study of | IARC coordinated study of | ||||||
|---|---|---|---|---|---|---|---|---|
| Leukemia |
Thyroid |
Leukemia |
Thyroid |
|||||
| Mean | GM | Mean | GM | Mean | GM | Mean | GM | |
| Number of study subjects | 1000 | 348 | 357 | 530 | ||||
| External irradiation during mission (RADRUE) | 92 | 14 | 116 | 12 | 45 | 37 | 29 | 24 |
| Exposure to 131I during mission | — | — | 23 | 3.5 | — | — | 39 | 16 |
| Exposure to short-lived I and Te during mission | — | — | 6 | 0.4 | — | — | — | — |
| External irradiation during residence | — | — | — | — | — | — | 5 | 1 |
| Exposure to 131I during residence | — | — | 47 | 3.7 | — | — | 182 | 70 |
| Total dose | 92 | 14 | 169 | 32 | 45 | 37 | 175 | 74 |
aRed bone-marrow dose (Chumak et al 2015). bPreliminary thyroid dose estimates for a fraction of the study subjects as of October 2014; the study is in progress (Chumak 2016). cBone-marrow dose (Kesminiene et al 2008). dThyroid dose (Kesminiene et al 2012).
Table 5. Distribution of the GSDs attached to the individual stochastic doses calculated by RADRUE for the subjects of the Ukrainian–American and IARC-coordinated studies of leukemia and thyroid cancer among Chernobyl cleanup workers (adapted with permission from Kryuchkov et al (2009), Chumak et al (2015)).
| GSD interval | Ukrainian–American study of | IARC-coordinated study of | ||||||
|---|---|---|---|---|---|---|---|---|
| Leukemia |
Thyroid |
Leukemia |
Thyroid |
|||||
| N | % | N | % | N | % | N | % | |
| <1.5 | 142 | 14.2 | 49 | 14.1 | 81 | 22.8 | 134 | 25.3 |
| 1.5–1.99 | 482 | 48.2 | 155 | 44.5 | 180 | 50.6 | 224 | 42.3 |
| 2.0–2.49 | 212 | 21.2 | 77 | 22.1 | 52 | 14.6 | 120 | 22.6 |
| 2.5–2.99 | 88 | 8.8 | 28 | 8.0 | 33 | 9.3 | 45 | 8.5 |
| 3.0–3.5 | 45 | 4.5 | 16 | 4.6 | 6 | 1.7 | 5 | 0.9 |
| 3.5 + | 31 | 3.1 | 23 | 6.6 | 4 | 1.1 | 2 | 0.4 |
| Mean GSD for the study | 2.0 | 2.1 | 1.9 | 1.9 | ||||
aBone-marrow dose. bThyroid dose. cPreliminary estimates for a fraction of the study subjects as of October 2014; the study is in progress (Chumak 2016).
3.2.2. IARC-coordinated study of hematological malignancies in cleanup workers from the Baltic States, Belarus and Russia.
A nested case-control study of hematological malignancies was conducted in cohorts of about 66 000 Chernobyl cleanup workers of 1986–1987 from Belarus, 65 000 from Russia and 15 000 from the Baltic countries. A total of 70 cases (40 leukemias, 20 non-Hodgkin lymphomas and ten other malignancies of lymphoid and hematopoietic tissue) and 287 matched controls were included in the study (Kesminiene et al 2008). The arithmetic means of the individual stochastic estimates of the bone-marrow doses among the study subjects ranged from 0.007–657 mGy (table 4). The GSDs of the individual stochastic external doses varied from 1.2–4.0 with a mean equal to 1.9 (table 5).
3.3. Category 2: occupational studies of thyroid cancer among Chernobyl cleanup workers
We considered here:
- 1.The IARC-coordinated study of thyroid cancer in cleanup workers from the Baltic countries, Belarus and Russia, and
- 2.The NCI-coordinated study of thyroid cancer in Ukrainian cleanup workers.
3.3.1. IARC-coordinated study of thyroid cancer in cleanup workers from the Baltic States, Belarus and Russia.
A collaborative case-control study nested within the cohorts of Belarusian, Russian and the Baltic cleanup workers was conducted by IARC to evaluate the radiation-induced risk of thyroid cancer (Kesminiene et al 2012). The study included 107 cases and 423 controls. In this study, in addition to the doses due to external irradiation, thyroid doses were also reconstructed for the following exposure pathways:
- Intake of 131I via inhalation during the period of work as a cleanup worker was calculated for the six study subjects who worked on the industrial site during the first 10 d after the accident;
- Inhalation of short-lived iodine and tellurium isotopes during the cleanup mission was estimated using the approach developed for the population of the 30 km zone around the Chernobyl nuclear power plant (Gavrilin et al 2004); and
- Intake of 131I with locally produced foodstuffs during residence between 26 April and 30 June 1986. Cleanup workers who were residents of the southeastern part of Belarus also received non-negligible doses at their places of residence if they lived in highly contaminated areas and consumed locally produced milk and/or vegetables.
The approach for the reconstruction of thyroid doses due to 131I was developed and validated by the results of direct thyroid measurements taken between 30 April 1986 and 5 May 1986 in a group of 624 early cleanup workers. For this purpose, the values of 131I activity in the thyroids were calculated with the approach used in the case-control study and then compared with those derived from the direct thyroid measurements. The mean of the ratios of those measured to the calculated activities was found to be 0.8 ± 1.1 and the median of the ratios was 0.5. The modeled doses from 131I inhalation for the study subjects were then calibrated against the median of the ratios of those measured to the calculated 131I activity in the thyroids of the group of 624 cleanup workers.
An estimation of the thyroid doses during residence and of their uncertainties was carried out using models developed previously for calculating the average thyroid doses due to 131I intake in adults who resided in the contaminated settlements of Belarus (Gavrilin et al 2004, Drozdovitch et al 2010). Such doses were not calculated for the Russian and the Baltic cleanup workers, who were sent on mission from distant areas with low or no contamination. The validity of the modeled thyroid doses was checked by comparison with the instrumental doses. The study subjects from Belarus resided in 33 settlements, where direct measurements of 131I activities in the thyroid were performed in May and the beginning of June 1986. Calculated residential thyroid doses from 131I intake were compared with the mean thyroid doses in residential settlements derived from direct measurements of 131I activities in the thyroid (figure 8). The mean of the ratios of the modeled-to-instrumental thyroid doses from 131I intake was 1.2 ± 0.5 and the median of the ratios was 1.1.
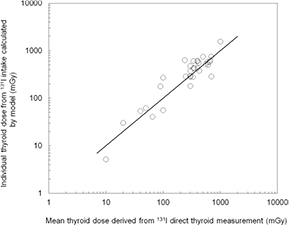
Figure 8. Comparison of thyroid doses from 131I intake for 33 subjects of the IARC-coordinated study of thyroid cancer in cleanup workers from Belarus, Russia and the Baltic countries: individual modeled versus mean settlement-specific dose for adults derived from direct thyroid measurements.
Download figure:
Standard image High-resolution imageThyroid doses from different exposure pathways estimated in this study are shown in table 4. It should be noted that only doses due to external irradiation during mission, which were calculated using RADRUE, are given for all study subjects. For other exposure pathways mean and GM of doses are shown only for the study subjects who were exposed to that exposure pathway. As can be seen from the table, for Belarusian cleanup workers exposure from 131I intake during residence was the main contributor to the overall mean thyroid dose.
The GSDs of the individual stochastic external doses calculated by RADRUE varied from 1.1–5.8 with a mean of 1.9 (table 5), while for the residential doses from 131I intake GSDs varied from 1.9–2.5 with a mean of 2.2 (not shown). Doses from external radiation and 131I intake were found to be independent of each other, because the approach to estimate these doses differed considerably, and little correlation was found between the arithmetic means of the individual stochastic dose estimates from both sources (Spearman's rank correlation coefficient: rs = 0.096). It should be noted that uncertainty in the thyroid doses due to 131I intake during residence was evaluated taking into account the separation of shared and unshared errors in the dosimetry model.
3.3.2. Ukrainian-NCI study of thyroid cancer in cleanup workers.
The Research Center for Radiation Medicine (Kyiv, Ukraine) in collaboration with the U.S. (NCI) is conducting a case-control study of thyroid cancer nested in a cohort of Ukrainian cleanup workers. In this study, in addition to the doses due to external irradiation, the thyroid doses are also being reconstructed, as in the IARC-coordinated study, for (a) the intake of 131I and short-lived iodine and tellurium isotopes via inhalation during the period of work as a cleanup worker, and (b) the intake of 131I with locally produced foodstuffs during residence. Some cleanup workers, who were residents of the northern part of Ukraine, might have received non-negligible doses at their places of residence, while consuming locally produced milk and/or vegetables.
Approaches for the reconstruction of thyroid doses due to the intake of 131I and short-lived iodine and tellurium isotopes via inhalation during the period of work as a cleanup worker were the same as in the IARC-coordinated study of thyroid cancer. To estimate residential exposure from the 131I intake, the method developed by Likhtarov et al (2005) to estimate the thyroid doses in the population in the absence of direct thyroid measurements was used.
Thyroid doses from different exposure pathways estimated in this study are shown in table 4. As can be seen from the table, external irradiation during the cleanup mission was, on average, the main contributor to the thyroid dose. However, some cleanup workers received high doses (up to a few Gy) from 131I intake from cows' milk at their places of residence between 26 April and 30 June 1986, as they lived in highly contaminated areas in a 30 km zone around the Chernobyl accident site. It should be noted that the dose estimates are preliminary as the study is ongoing.
The GSDs (intrinsic uncertainty) of the individual stochastic external doses varied from 1.2–7.0 with a mean equal to 2.1 (table 5), while for the residential doses from 131I intake GSDs varied from 1.8–4.9 with a mean of 2.5 (not shown). Doses from external radiation and 131I intake were found to be independent, as the approach used to estimate these differed considerably and because little correlation was found between the arithmetic means of the individual stochastic dose estimates from both sources (rs = −0.02). Uncertainty in the thyroid doses due to the 131I intake during residence was evaluated, taking into account the separation of shared and unshared errors in the dosimetry model.
3.4. Category 3: occupational study of cataract among Chernobyl cleanup workers
The only study in this category is the Ukrainian–American Chernobyl Ocular Study (UACOS), which is a cohort study among Chernobyl cleanup workers who were on mission in 1986–1987. The 8607 cohort members had two ophthalmic examinations with a two-year interval in between (Worgul et al 2007). Study endpoints included both mature cataracts and pre-cataract changes (vacuoles, polychromatic sheen, etc). The size of the cohort precluded the individual dose reconstruction for the study participants. Only individuals with available dosimetric information were included in a study with a further revision and validation of their dose records. The study cohort included mainly (a) military cleanup workers with ODRs stored in the State Chernobyl Registry of Ukraine (SRU), (b) people for whom doses had been reconstructed analytically (using a time-and-motion method), and (c) those for whom doses were reconstructed using EPR dosimetry measurements of tooth enamel. The above-listed sources of dosimetric information dealt with external gamma radiation only, plus uncertainty and possible bias of existing dose records had to be evaluated and, if needed, adjusted. Therefore, the plan of dose reconstruction consisted of two steps. In the first step, all types of dosimetric data were recalibrated against EPR dosimetry measurements of tooth enamel (Chumak et al 2005). The latter protocol encompassed features aimed at an accurate and unbiased evaluation of the doses: only samples with sufficient amount of dental enamel at the buccal and lingual parts of a molar were used for analysis; for each tooth, doses to both parts of a tooth were reconstructed, taking into account possible dental x-ray contributions. For each sample, its individual sensitivity was calibrated by an additive dose method. As a result, the accuracy of the doses based on the EPR dosimetry method (±25 mSv for doses below 250 mSv and 10% for higher doses) (Chumak et al 2005) was superior compared to any other concerned dosimetric data. Consequently, an application of this EPR dosimetry protocol made the retrospective recalibration of existing dose records possible. It was found that ODRs for military cleanup workers overestimated actual exposure by a factor of about 2.2 (Chumak et al 2007). This resulted in a retrospective adjustment of ODRs. It should also be mentioned that a separate sub-study of the statistical features of ODR distributions in military cleanup workers (Chumak et al 2000) led to the conclusion that intentional falsification of doses, if any, affected no more than 10% of this cohort, thus addressing a concern caused by the unusual shape of the dose distribution for military cleanup workers. As a result of the first step of the dosimetric effort, a corrected external photon dose to the lens along with an estimate of the associated uncertainty (GSD) was assigned to each cohort member.
The next step produced the total (both β and γ) dose to the lens. This was achieved via the application of a subject-specific conversion coefficient, relating β dose to the dose of γ radiation. These ratios were calculated using a Monte Carlo method (MCNP-4B code) for specific environments and source energies (irradiation situations) (Chumak et al 2007). The parameters influencing the β-to-γ ratio were: time after the accident (due to various decay times of the main β- and γ-emitters, this ratio significantly evolved with time reaching maximum about one year after the accident), the use of protective goggles, the work environment (i.e. size of a room, presence of windows, and roughness of surfaces). In order to obtain this information, a large proportion of the study subjects were interviewed during the second ophthalmic examination, with a specially designed short questionnaire; for those subjects missing this questionnaire data, the likelihood of each of the options was weighted and then used as a stochastic variable in the simulation of the resulting (β + γ) dose. This means that for each subject the stochastic simulation was performed using uncertainties of the γ dose, situation-specific conversion coefficients and the weights of various exposure situations as inputs of the model. As a result, individual lens doses were estimated for all the study subjects. The distribution of the associated individual uncertainties (GSDs) is presented in figure 9. As can be seen from the figure, individual uncertainties of dose estimates vary a lot depending on a number of factors (accuracy of the original dose record, level of certainty regarding conditions of exposure during cleanup, imprecision of conversion from γ to the total lens dose, etc), but in general are at an acceptable level (most of subjects had GSDs of individual dose distribution between 1.9 and 2.2). Further improvement of dose estimates is possible by applying a more realistic model (eye phantom, geometry of exposure) for evaluation of the β-to-γ conversion coefficients as well as by more specific adjustment of the existing dose records by applying narrower classes for retrospective calibration. Nevertheless, the dosimetry system used for the epidemiological analysis of radiation-induced lens opacities gave a first approximation of the dose estimates to the lens with a sufficient degree of accuracy and confidentiality (Chumak et al 2007, Worgul et al 2007).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Figure 9. Distribution of GSDs of individual dose distributions for 8607 study subjects of the Ukrainian–American Chernobyl Ocular Study (UACOS).
Download figure:
Standard image High-resolution image{kind=link}
4. Discussion
4.1. Comparison with other analytical studies in low-dose-level radiation epidemiology
To place the dosimetric approaches used in post-Chernobyl studies within the general picture of dose reconstruction applied in radiation studies, it is necessary to compare those with other analytical studies of low-dose radiation in terms of the uncertainty and reliability of dose estimates. Occupational, medical and environmental studies, all non-related to the Chernobyl accident, are considered in turn in the sections below.
4.1.1. Dosimetry in occupational exposure studies.
Dosimetry in occupational studies has an advantage, because personnel having contact with ionizing radiation were monitored using personal dosimeters. However, occupational doses are also associated with uncertainties.
A study of errors in the recorded doses was conducted as a part of the 15 country nuclear industry workers' study (Cardis et al 2007) to evaluate the comparability of the recorded dose estimates across facilities and time, and to identify and quantify the sources of bias and uncertainties in the dose estimates (Thierry-Chef et al 2007). The major sources of errors in external radiation doses were found to be dosimetry technology, exposure conditions of the workplace, and calibration practices. These sources of systematic errors were characterized and quantified. Although the sources of the dose errors (mainly shared) were well quantified in the study, multiple dose realizations were calculated not for the entire cohort, because of the cohort size of 407 391 nuclear industry workers, but only for the Oak Ridge National Laboratory (ORNL), one of the study facilities included in the 15 country study (Stayner et al 2007). Monte Carlo simulations were used for this facility to randomly select a set of bias factors from the assigned distributions. The resulting bias factors were then used to estimate the annual 'corrected' doses for each worker in the study by dividing their annual recorded dose by the appropriate sampled bias factor. Ten thousand individual stochastic annual doses were generated for each individual in the ORNL cohort and used for estimating an excess relative risk and its confidence interval that reflects both the statistical sampling error and uncertainty in the measurement of exposures (Stayner et al 2007). Another source of uncertainties is the difficulties in accounting for exposure due to lower-energy photons and neutrons and from the intake of radionuclides. In particular, in the 15 country study workers with a potential for a substantial dose from these sources of exposure (⩾10% of their whole-body dose) were flagged and excluded from the main epidemiological analyses (Thierry-Chef et al 2007).
Updated and expanded methods of occupational exposure assessment were used in the International Nuclear Workers Study (INWORKS) conducted in France, the United Kingdom and the United States of America in a cohort of 308 297 workers (Thierry-Chef et al 2015). This approach accounts for differences in dosimeter response to predominant workplace energy and geometry of exposure, and for sex-specific dose conversion coefficients recently published by the ICRP (ICRP 2010). Workers potentially exposed to neutrons (neutron dose exceeded 10% of the external dose) and with internal contamination were identified and flagged (Thierry-Chef et al 2015). As in the 15 country study, individual stochastic doses were not calculated for the cohort.
The most comprehensive uncertainty assessment in the doses reconstructed for the studies of occupational exposure was done for the study of 110 374 U.S. radiologic technologists (USRT study) (Sigurdson et al 2003). The previous USRT dosimetry system (Simon et al 2006a) was revised and significant improvements were made to estimate the annual and cumulative individual organ doses received by medical radiologic technologists (Simon et al 2014). The USRT dosimetry system was designed to account for the separation of the shared and unshared errors, and allowed for the production of 1000 realizations of the cohort dose. Uncertainties in the organ doses for each study subject are characterized by the GSD of 1000 individual stochastic doses. For example, the GSDs of breast doses among the female study subjects varied from 1.2–6.4 (Simon et al 2014).
Obviously, there are limitations in occupational dosimetry including, among other factors, the processing of dosimetry readings below the detection limit, the lack of measurements in earlier years, and not accounting for neutron doses and doses from the intake of radionuclides.
4.1.2. Dosimetry in medical exposure studies.
Different measures of exposure have been used in the epidemiological studies of low-level medical exposure, in particular, of exposure to patients from computed tomography (CT) procedures. Some studies did not estimate the actual radiation exposure from each CT scan, because of the absence of the patients' data for dose assessment. In some of studies, the number of CT scans was used as a measure of a person's radiation exposure (e.g. Huang et al 2014). In others, an effective dose, not an absorbed dose, was used to assess risk estimates (e.g. in Mathews et al 2013). In the studies with the most advanced dosimetry, an absorbed dose in the target organs was reconstructed for the study subjects based either on a CT scan-dose matrix or on CT-model and machine settings (e.g. Pearce et al 2012, Meulepas et al 2014).
The actual absorbed doses from CT scans can vary substantially depending on the patient's age, sex, equipment type, shape and size of the patient's body, the use of contrast, protocols of scanning, purpose of examination, etc. Data for the machine settings that also influence the dose, such as milliampere seconds and peak kilovoltage, are typically not available for each of the study participants. Therefore, a dose that is typically averaged per scan by site, years of scan and by age, is used to characterize individual exposure (Mathews et al 2013). Other sources of uncertainty include the absence of records on repeated scans that were done because of patient movements; missing doses for CT examinations with unknown anatomical areas; and incomplete radiology data (Journy et al 2015, Krille et al 2015).
Although radiation exposure assessment in the medical exposure studies with the most advanced dosimetry (e.g. Pearce et al 2012, Meulepas et al 2014) is quite accurate compared to that in other areas of radiation epidemiology, uncertainties in the studies of low-level medical exposure are acknowledged, but not numerically estimated.
4.1.3. Dosimetry in environmental exposure studies (other than Chernobyl-related).
Uncertainties in the studies of environmental exposure, where thyroid doses were based only on modeling, are typically higher than those reported in the post-Chernobyl thyroid dose estimates based on direct thyroid measurements. A mean GSD of 2.2 (range 1.6–5.4) was reported by Kopecky et al (2004) for thyroid doses reconstructed for the participants of the Hanford thyroid disease study. For thyroid doses reconstructed in the Utah thyroid cohort study, as a consequence of radioactive fallout from atmospheric nuclear weapons tests, the GSDs varied from 1.5–8.5 with the majority of values lying in the range from 2–3 (Simon et al 2006b). A comprehensive dose reconstruction using the 2DMC method (Simon et al 2015) was conducted recently for a cohort of 2376 individuals exposed at age <21 years to the Semipalatinsk Nuclear Test Site fallout in Kazakhstan (Land et al 2015). The GSDs of individual stochastic thyroid doses due to the intake of radioiodines varied up to 9.3 with a mean GSD of 3.7 and the majority of values lying in the range from 3–4 (derived from Land et al 2015).
4.2. Gaps in methodology and suggestions for improvement of post-Chernobyl dosimetry
The characteristics of the dosimetry methods and the main dosimetry results of the post-Chernobyl analytic studies are summarized in table 6.
Table 6. Summary of dosimetry of post-Chernobyl analytical epidemiological studies.
| Design | Country | Age at exposure (years) | N study subjects | Use of measurements | Target organ, exposure pathway | Dose (Gy) | Uncertainty | References | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | Median | Max | Shared | Mean GSD | Range of GSD | |||||||
| Environmental studies of thyroid cancer and other thyroid diseases in general population: | ||||||||||||
| Studies with individually-based radiation measurements and evaluated uncertainties in doses (Category 1) | ||||||||||||
| Cohort | Belarus | 0–18 | 11 732 | Basis for dose (100%) | Thyroid, 131I | 0.68 | 0.27 | 39 | Y | 1.8 | 1.3–5.1 | Drozdovitch et al (2013b, 2015) |
| Cohort | Ukraine | 0–18 | 13 204 | Basis for dose (100%) | Thyroid, 131I | 0.65 | 0.19 | 42 | Y | 1.6 | 1.3–10.6 | Likhtarov et al (2014) |
| Studies with modeling doses and evaluated uncertainties in doses (Category 2) | ||||||||||||
| Case-control | Belarus, Russia | 0–18 | 1615 | Basis for dosimetry model | Thyroid, 131I | 0.49 | 0.21 | 9.5 | Y | 2.2 | 1.7–4.0 | Drozdovitch et al (2010) |
| Case-control | Russia | 0–19 | 198 | Basis for dosimetry model | Thyroid, 131I | — | 0.044/ 0.016 |
2.7 | N | 2.2 | 1.8–3.5 | Kopecky et al (2006) |
| Stepanenko et al (2004) | ||||||||||||
| Studies with modeling doses and unquantified uncertainties in doses (Category 3) | ||||||||||||
| Case-control | Belarus | 0–15 | 321 | Basis for dosimetry model | Thyroid, 131I | 0.3 | 0.11 | 4.3 | — | — | — | Gavrilin et al (2004) |
| Minenko et al (2006) | ||||||||||||
| Cohort | Ukraine | In utero | 2582 | Basis for dose (30%) | Thyroid, 131I | 0.072 | 0.012 | 3.2 | — | — | — | Likhtarov et al (2011) |
| Occupational studies in Chernobyl cleanup workers | ||||||||||||
| Studies of leukemia and other hematological malignancies with RADRUE dose estimates and evaluated uncertainties in doses (Category 1) | ||||||||||||
| Nested case-control | Ukraine | 18 + | 1000 | RADRUE validation | Bone marrow, external | 0.092 | 0.014 | 3.3 | N | 2.0 | 1.2–5.9 | Chumak et al (2008, 2015) |
| Nested case-control | Belarus, Russia, Baltic countries | 18 + | 357 | RADRUE validation | Bone marrow, external | 0.045 | 0.037 | 0.66 | N | 1.9 | 1.2–4.0 | Kesminiene et al (2008) |
| Kryuchkov et al (2009) | ||||||||||||
| Studies of thyroid cancer with RADRUE dose estimates and evaluated uncertainties in doses (Category 2) | ||||||||||||
| Nested case-control |
Ukraine | 18 + | 348 | RADRUE validation | Thyroid, external, 131I | 0.17 | 0.032 | 2.3 | N | 2.0 |
1.2–7.0 |
— |
| Y |
2.5 |
1.8–4.9 |
||||||||||
| Nested case-control | Belarus, Russia, Baltic countries | 18 + | 530 | RADRUE validation | Thyroid, external, 131I | 0.18 | 0.069 | 3.3 | N | 1.9 |
1.1–5.8 |
Kesminiene et al (2012) |
| Y |
2.2 |
1.9–2.5 |
||||||||||
| Study of cataract with ODR-adjusted dose estimates and evaluated uncertainties in doses (Category 3) | ||||||||||||
| Cohort | Ukraine | 18 + | 8607 | ODR dose adjustment | Lens, external, β-particles | 0.16 | 0.12 | 2.3 | N | 2.2 | 1.01–3.2 | Chumak et al (2007) |
aCases/controls. bPreliminary thyroid dose estimates for a fraction of the study subjects as of October 2014; the study is in progress (Chumak 2016). cThyroid dose due to external irradiation. dThyroid dose due to 131I intake at places of residence between 26 April and 30 June 1986.
4.2.1. Environmental studies.
The discussion on environmental studies is split into two parts: those that deal with thyroid cancer and other thyroid diseases, where 131I is the main radionuclide contributing to the thyroid dose, and the studies of all other cancer endpoints, for which external irradiation and internal irradiation due to ingestion of caesium isotopes play a major role.
4.2.1.1. Studies of thyroid cancer and other thyroid diseases.
As discussed above, in the two cohort studies that include subjects with direct thyroid measurements performed within two months after the accident, the estimation of the thyroid dose is based on the results of those measurements and on an ecological model providing the variation of the thyroid activities of 131I both before and after the direct thyroid measurements. The approach was validated using two sets of thyroid dose estimates: one that included the results of the direct thyroid measurements, and another that excludes them. The ratio of the two dose estimates for a given subject, called the scaling factor, provides an estimate of the validity of the ecological model, assuming that the direct thyroid measurement result is correct. The distribution of the scaling factors for the Belarusian subjects, shown in figure 5, is very wide, with a GSD of about 5; in addition, a bias in the scaling factor was observed in the Belarusian subjects. In the Ukrainian study, the distribution of the scaling factors is also very wide, but there is no substantial bias.
A thorough analysis of the following parameter values included in the calculation of the scaling factor is recommended:
- The exposure rate or count rate measured during the direct thyroid measurement and its conversion into the thyroid dose rate, the parameter values used in the ecological model to simulate the 131I transfer from deposition to thyroid activity, including, among others, a thorough analysis of the available measurements of 129I in soil, and of 131I (or total beta activity) in milk. In that respect, it should be noted that a special effort was made in Belarus to: (1) collect all environmental radiation and meteorological data available for the first weeks or months after the accident, including (a) the results of 131I measurements in the soil, grass and cow's milk (Drozdovitch et al 1997, 2013a); (b) the results of total beta-activity measurements to evaluate levels of 131I concentration in cows' milk (Drozdovitch et al 2006, Khrutchinsky et al 2009); and (c) 129I measurements in soil samples from 37 Belarusian settlements to validate the region-specific ratios of 131I-to137Cs activities in ground deposition (Straume et al 1996, 2006); (2) validate these measurements and include them in an electronic database; and (3) use them, at least in part, to derive site-specific parameter values to be used in the ecological model. It is hoped that the Belarusian database will be fully processed and that similar efforts will be made in Ukraine and in Russia;
- The responses provided by the subjects during their personal interviews on residence history and dietary habits.
This analysis would lead to the development of an ecological model that predicts with no bias and improved accuracy the thyroid doses of the subjects. This 'ideal' ecological model could substantially improve the dose estimates for the subjects of epidemiologic studies that include a limited number of subjects with direct thyroid measurement.
Consideration could also be given to an evaluation of the validity of the current methodology used to estimate the instrumental thyroid doses and their uncertainties. As implied in section 2.1 above, an assumption is made that the relative shape of the variation of 131I activity in the thyroid with time is correct, so an adjustment at the time of measurement, which includes replacing the calculated 131I thyroid activity at the time of measurement with the measured value, also applies to any other time after the accident. This is due to the fact that the temporal variation of the 131I thyroidal activity resulting from the consumption of each of the main foodstuffs contributing to the thyroid dose (milk, milk products, and leafy vegetables) is, to a good approximation, proportional to the same function of time. Therefore, the assumption that the relative shape of the variation of 131I activities in the thyroid with time is correct appears to be valid under conditions of continuous residence in the same settlement during the first two months after the accident and the daily consumption of foodstuffs from the same sources. However, in the event of changes in the parameter values that have an additive effect, such as relocation to a settlement with a different 131I ground deposition density, the assumption is no longer valid and both the thyroid dose estimate and its uncertainty are modified to some extent. Research is needed to investigate the influence of relocation and dietary changes on the current thyroid dose estimates and their uncertainties.
4.2.1.2. Studies of other endpoints.
The doses for other endpoints (breast cancer, leukemia, etc) have two major components: (1) external irradiation, resulting in the short-term from a radionuclide mix (132Te–132I, 140Ba–140La, 95Zr–95Nb, 131I, etc) and in the long term from 134Cs and 137Cs, and (2) internal irradiation, resulting essentially from the intake of 134Cs and 137Cs:
- Doses from external irradiation: the two areas that appear to need further investigation are: (1) the estimation of the doses received in urban environments and, in particular, in large cities, where radionuclides are expected to have been removed more efficiently than in rural areas and where buildings provide more effective shielding. For that purpose, it would be helpful to analyze the outdoor and indoor measurements of exposure rates that were made throughout the affected areas, and (2) the estimation of the long-term variation with time of the vertical profile of 137Cs in the soils of rural areas, as this has an effect on the doses predicted over a large time span.
- Doses from the intake of 134Cs and 137Cs: it would be useful to develop an ecological model consistent with the available whole-body measurements and the available Cs concentrations in milk.
4.2.2. Occupational studies.
4.2.2.1. Leukemia studies.
The bone-marrow doses used in the studies of leukemia and other hematological malignancies are due to external irradiation. Until now, they have been obtained using the RADRUE method, which presents the advantage of being applicable to any worker, whether dead or alive. The weaknesses of the RADRUE method are that: (1) it is time consuming, and (2) the uncertainties in the resulting dose estimates could be quite large, because essential input data, obtained by means of personal interviews, particularly if they are performed more than 30 years after the accident, may be unreliable and are very difficult to evaluate. Future work could include:
- A thorough analysis of the ODRs and of the measured daily dose rates, in order to determine conditions under which the 'improved' or 'calibrated' ODRs could replace the RADRUE dose estimation in the cleanup workers' studies;
- An extensive effort to validate the ODRs by means of a comparison with the results of currently available EPR and fluorescence in situ hybridization (FISH) measurements, and the recommendation to perform more EPR and FISH measurements, if they appear to be justified; and
- The development of a method to evaluate the uncertainties related to the poor quality of the questionnaire responses.
4.2.2.2. Studies of thyroid cancer.
For early workers who were present on the Chernobyl site from the time of the accident until 10 May, it is very important to estimate the thyroid doses from the intake of 131I. Unfortunately, only a few measurements of 131I were made during that period of time, with the exception of a set of 624 direct thyroid measurements that were made a few days after the accident. Because relatively detailed information on the whereabouts of the measured workers is also available, it is judged important to include in the future program of work a detailed analysis of the data related to those 624 early cleanup workers.
5. Summary and conclusions
This paper was prepared to respond to the discussion in the scientific community on the reliability of the individual dose estimates used in analytical epidemiological studies related to the Chernobyl accident. To evaluate the validity of those doubts, we thoroughly described and discussed the methods used to estimate individual doses and associated uncertainties in the most informative post-Chernobyl analytical epidemiological studies (i.e. cohort or case-control).
This paper evidences that individual doses for Chernobyl-related analytical epidemiological studies have been calculated with a relatively high degree of reliability and well-characterized uncertainties, and that they compare favorably with many other non-Chernobyl studies. The major strengths of the Chernobyl dosimetry studies include the use of a large number of individually-based or environmental measurements and extensive efforts to characterize dose uncertainties. However, some of the measurements should have been given more proper consideration. The costs and time associated with the implementation of the RADRUE method make this method difficult to apply in large cohort studies on cleanup workers and alternative approaches should, therefore, be considered. Appropriate accounting for questionnaire-related uncertainties (for example, those associated with the poor recall of the whereabouts of the cleanup workers during their mission at the Chernobyl site) needs to be addressed in further studies.
Funding
This paper was prepared within the framework of the European Commission Euratom FP7 grant No. 605302 'Cooperation on Chernobyl Health Research (CO-CHER)' coordinated by the International Agency for Research on Cancer (Lyon, France).
Acknowledgments
The authors gratefully acknowledge the contributions of the late Drs G W Beebe, G R Howe and E Ron to the design, setup and conduct of the studies considered in the paper. The authors also gratefully acknowledge the contributions of Drs L Anspaugh, D Bazyka, M Balonov, A Brenner, E Cardis, Y Gavrilin, G Goulko, M Hatch, V Khrouch, V Kryuchkov, L Kovgan, I Likhtarov, N Luckyanov, K Mabuchi, E Maceika, V Minenko, A Romanenko, S Shinkarev, V Stepanenko, M Tronko, P Voillequé, L Zablotska, I Zvonova, and many others to the epidemiologic and dosimetry methods applied in the reviewed studies.